














Report on Findings
HealthHIV’s Sixth Annual State of HIV Care™ National Survey identifies barriers that HIV care providers face in delivering care, captures their perspectives on existing resources, and highlights their experiences with achieving patient outcomes in 2024. These survey insights create vital education and training for the HIV care workforce and inform advocacy and research priorities for the coming year. The survey questions were developed using the HIV Care Continuum, a status-neutral framework that outlines the stages of HIV care. By framing the survey around this continuum, the survey ensures a comprehensive understanding of the interconnected nature of prevention and care in addressing HIV.
Download this Report
This report is available as a PDF document.
 Download PDF
Download PDF
Overview
The U.S. has set ambitious targets through the Ending the HIV Epidemic in the U.S. (EHE) initiative, aiming to reduce new HIV infections by 75% by 2025 and 90% by 2030, increase PrEP coverage to 50% by 2025, and ensure that 95% of newly diagnosed individuals are linked to medical care by 2025.1 Despite these goals, progress has been slow, with significant barriers hindering achievement.2 Although improvements in insurance coverage have been made over the past decade, largely due to Medicaid expansion under the Affordable Care Act (ACA), over 40% of working-age Americans remained underinsured in 2022.3, Complex insurance practices continue to create significant gaps in care, disproportionately impacting younger, Latinx/Hispanic, economically disadvantaged individuals, and those residing in the South—populations that also face increased vulnerability to HIV.3, 4 These overlapping social and health challenges underscore the critical role of HIV care in addressing broader syndemics, where interconnected social and medical issues compound the burden of disease and make comprehensive, equitable care even more essential. In 2023, nearly one-third of Americans lived in primary care Health Professional Shortage Areas, further exacerbating the national workforce shortages and burnout crises, which strain healthcare systems and hinder engagement in HIV prevention and treatment services.5
Previous State of HIV Care National Surveys have consistently identified similar challenges, such as workforce burnout, behavioral health concerns, HIV criminalization, and the social and political determinants of health. The recurrence of these issues emphasizes their persistent nature, especially with regard to funding constraints and insurance barriers. However, new findings from 2024 highlight some important developments. There has been a marked shift toward treatment innovation, with widespread adoption of long-acting injectables reflecting the growing enthusiasm among providers for novel strategies in HIV care. Despite this, there is heightened concern among participants about policies that reinforce stigma and increase barriers to care, particularly for populations disproportionately impacted by HIV. These policies exacerbate the inequities within the healthcare system, making it even more difficult to achieve the EHE goals.
This report, based on insights from frontline healthcare providers, offers a critical look at the current state of HIV care in the context of EHE objectives. Understanding the systemic gaps and challenges faced by healthcare professionals is crucial for informing strategies that will improve HIV prevention and treatment, ensuring progress toward the 2025 and 2030 targets for ending the HIV epidemic in the U.S.
The State of HIV Care
In asking respondents to capture the State of HIV Care in one word, “improving” emerged prominently at the center, symbolizing the significant advancements in treatment and support; encircling it are “evolving”, “progressing,” “lacking,” and “hopeful,” which together convey a nuanced picture of ongoing challenges, potential for growth, and a collective optimism for the future.
What is the State of HIV Care in one word?
 Download Graphic
Download GraphicData from the HealthHIV State of HIV Care™ Sixth Annual National Survey
HealthHIV.org/stateof/hivcare
Key Findings
- Workforce Shortages, Inadequate Compensation, and Burnout Create a Challenge to Quality HIV Care
Providers report that workforce shortages, inadequate compensation, and burnout are the primary barriers to quality care, underscoring an urgent need for increased funding and staffing support. - Providers Request Training on New Treatments and Health Equity
Clinicians and service providers emphasize the need for training in innovative HIV treatments, such as long-acting injectables, as well as guidance on addressing health disparities and navigating funding challenges. These areas are vital for improving care delivery and addressing systemic inequities. - Lack of Essential Behavioral Health Services Driving Gaps and Undermining Care for People with HIV
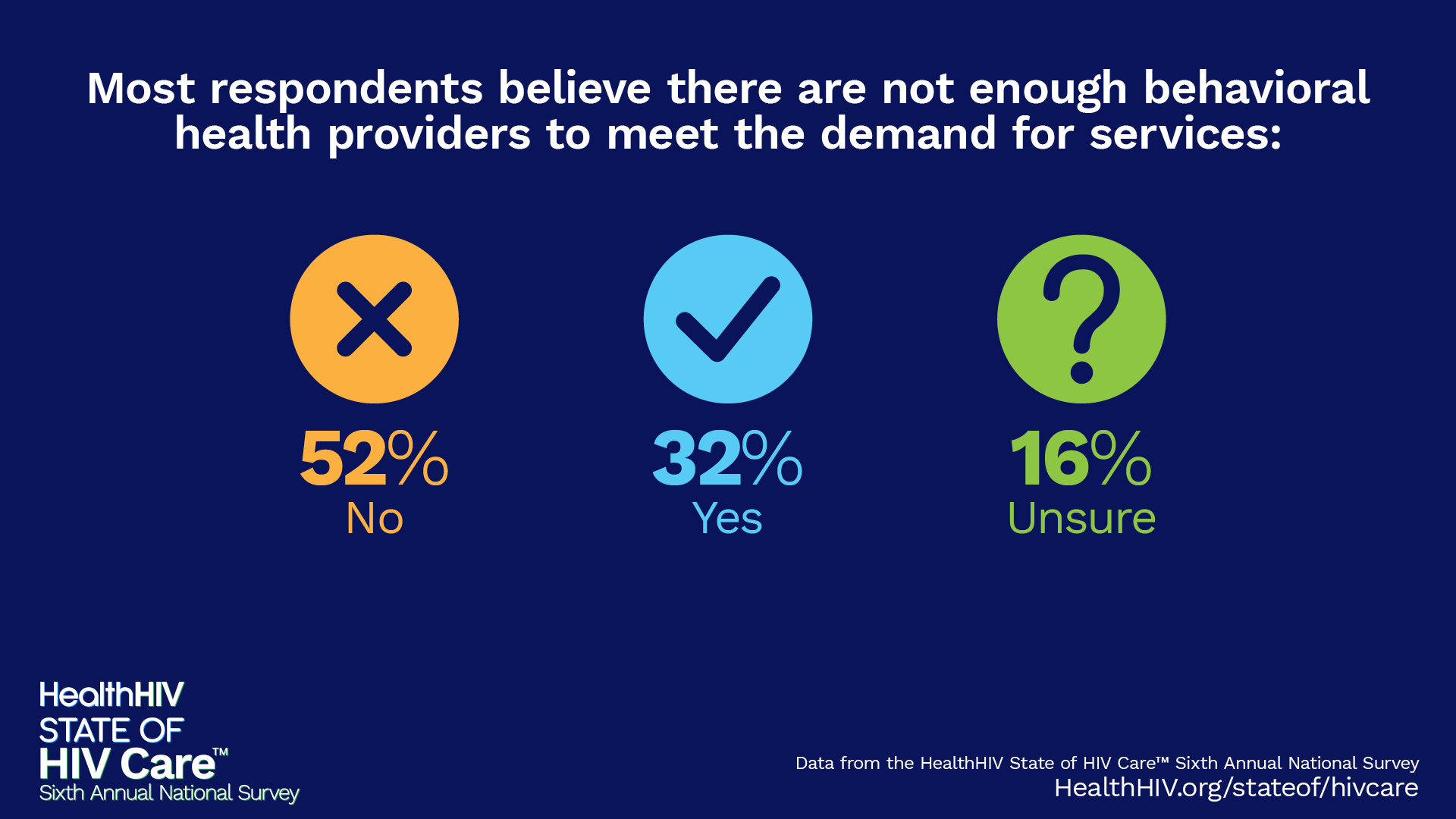
Many organizations are missing essential services, particularly in behavioral health and social services, resulting in the exclusion of social determinants of health from necessary care. Fewer than 30% of respondents offer services like childcare, inpatient detox, and crisis support, highlighting a national shortage of behavioral health care providers. This deficiency poses a barrier to meeting the broader health needs of people with HIV (PWH) and those at risk. - Ongoing Stigma Hindering Retention in HIV Care for Priority Populations
Stigma significantly complicates retention in HIV care, as many organizations struggle to provide sufficient behavioral health support. Fear of judgment and distrust in healthcare systems hinder access to care, especially for priority populations, including those experiencing homelessness and individuals who use substances. - Insurance Barriers Slowing Access to PrEP and HIV Care, Highlighting Need for Reform
Insurance barriers, such as formulary restrictions, high co-pays, and prior authorizations, delay access to ART and PrEP, disproportionately impacting priority groups. Providers face limitations in delivering care, and many lack familiarity with zero-cost-sharing guidelines for PrEP, emphasizing the need for policy reforms and targeted training to improve access and outcomes.
These findings reflect systemic challenges that the HIV care workforce faces, including the need for more comprehensive service offerings, expanded workforce training, and policy reform to reduce stigma and legal barriers in care provision.
About the Report
This report is structured to present a clear overview of the main findings and inferences from the HealthHIV Sixth National State of HIV Care™ survey, supported by relevant graphics that illustrate key trends and insights. The addendum contains all survey questions and detailed data to provide transparency and allow for deeper analysis, ensuring that those interested can review the underlying information that supports the report’s conclusions.
Participant Background
Total Respondents
966 professionals who provide HIV-related services across the care continuum.
Geographic Reach
Responses came from providers in 46 states, Puerto Rico, and the District of Columbia.
Healthcare Settings Represented
- Community-Based Organizations (CBOs)
- Community Health Centers
- Ryan White HIV/AIDS Program Clinics
- Health Department Clinics
Priority Populations Served
The majority of providers offer services to all listed priority groups, with particular emphasis on:
- People experiencing homelessness or who are unhoused
- Individuals with substance use disorders
- Non-English-speaking individuals
- Organizations located in urban areas
Survey Findings
State of the HIV Care Workforce
Workforce Crisis Deepens
Survey findings highlight a dire need for increased funding and staffing across the entire HIV care continuum. Providers from diverse professional backgrounds overwhelmingly report that staff shortages and inadequate compensation are the most pressing challenges facing the workforce. This marks the third consecutive State of HIV Care Survey where workforce shortages have been identified as one of the greatest barriers to effective HIV care, revealing a persistent crisis that threatens the future of care delivery.
Top three needs to improve HIV services:
 Download Graphic
Download Graphic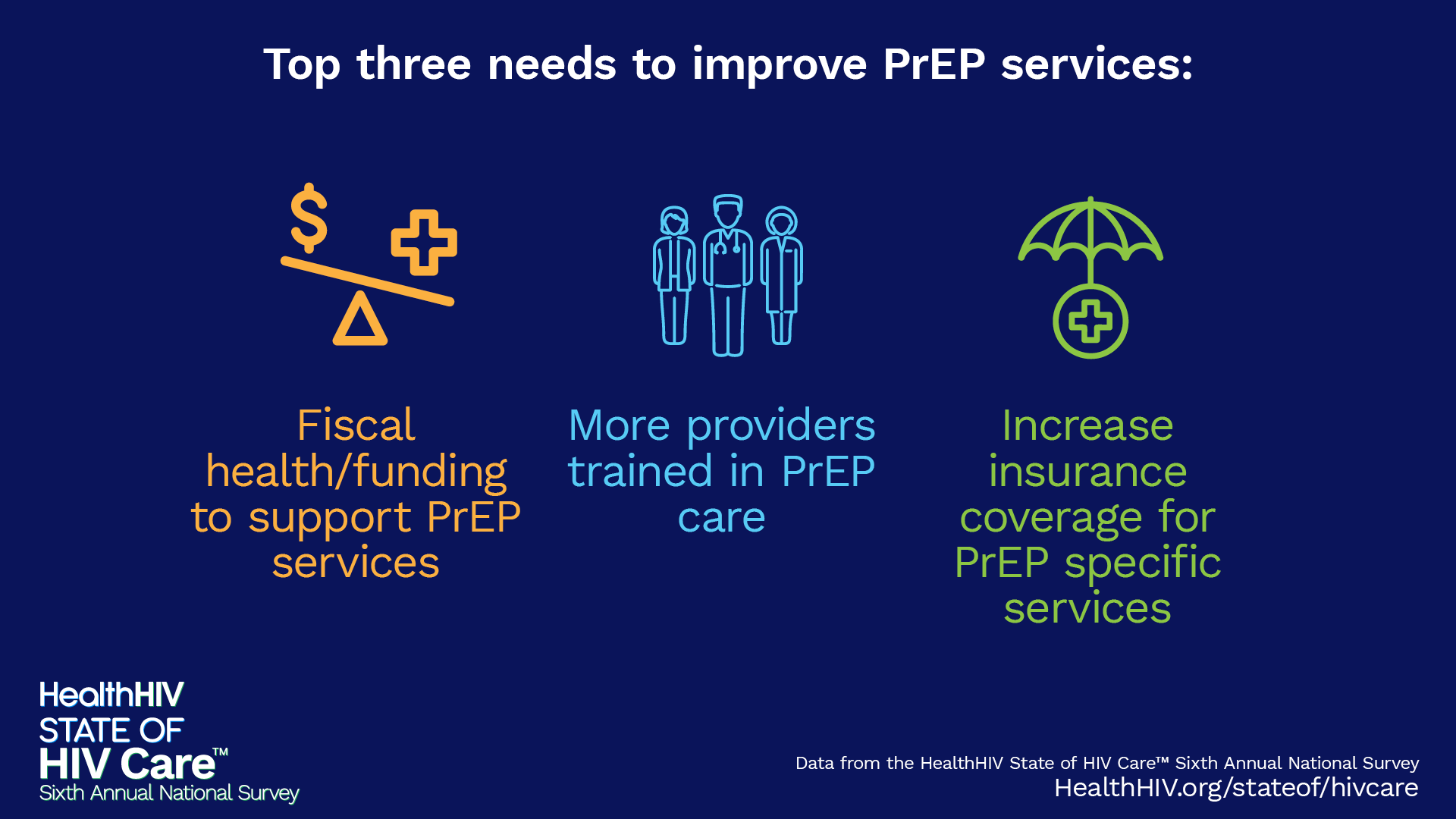 Download Graphic
Download Graphic Download Graphic
Download GraphicTop three health care topics for training:
Respondents identify health disparities and fiscal health as top healthcare topics for training, reflecting overall concerns about systemic inequities and program funding, present throughout the report.
 Download Graphic
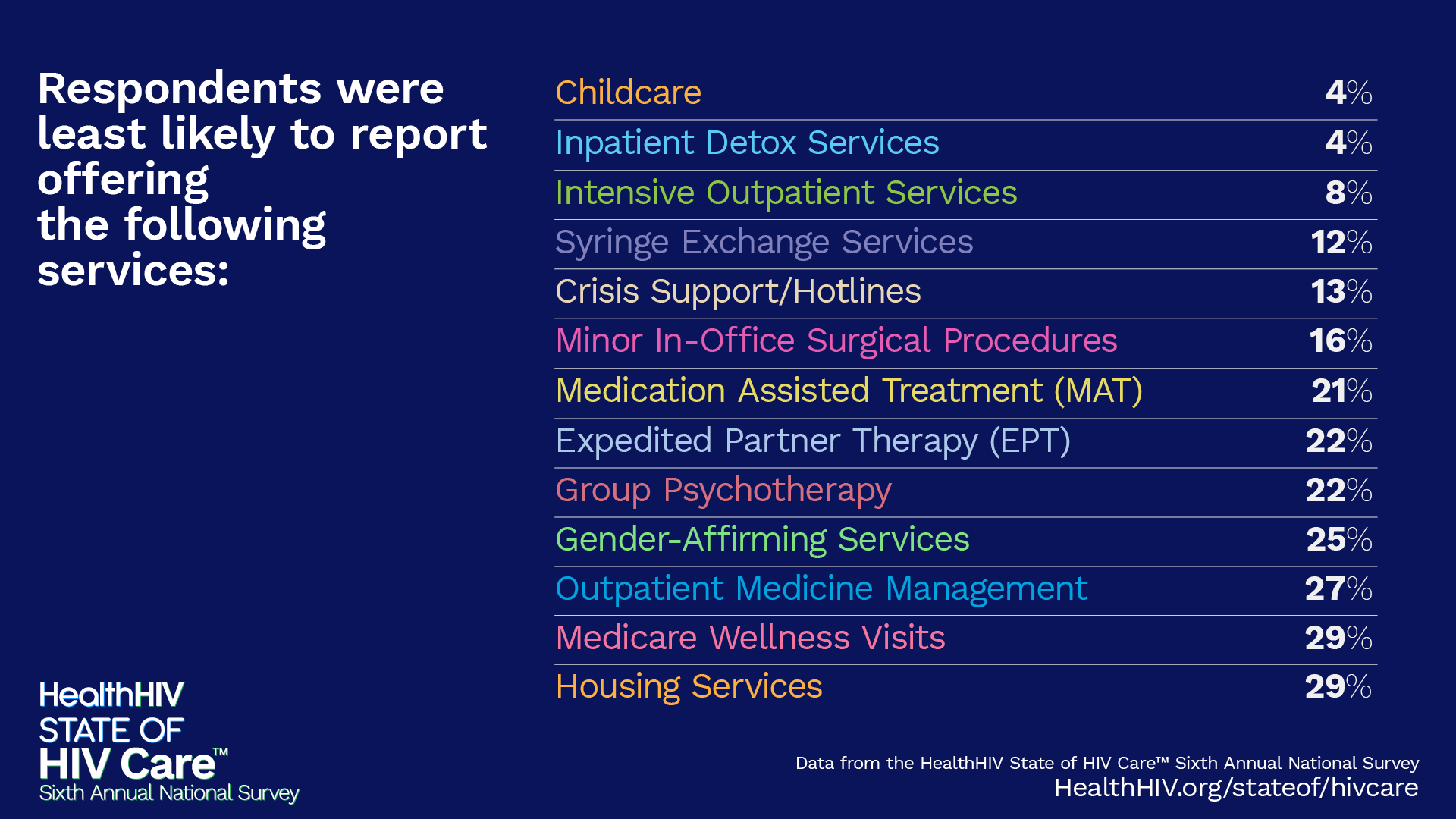
Download GraphicCritical Service Gaps Exposed
There are clear gaps in essential services across HIV, HCV care, sexual and behavioral health, and social determinants of health. Providers are least able to offer critical resources like childcare, inpatient detox services, Intensive Outpatient Services, syringe exchange programs, and crisis support—underscoring a nationwide shortage of behavioral health professionals and social services that leaves priority populations at risk.6
Respondents were least likely to report offering the following services:
 Download Graphic
Download GraphicMost timely and important HIV Care topics:
 Download Graphic
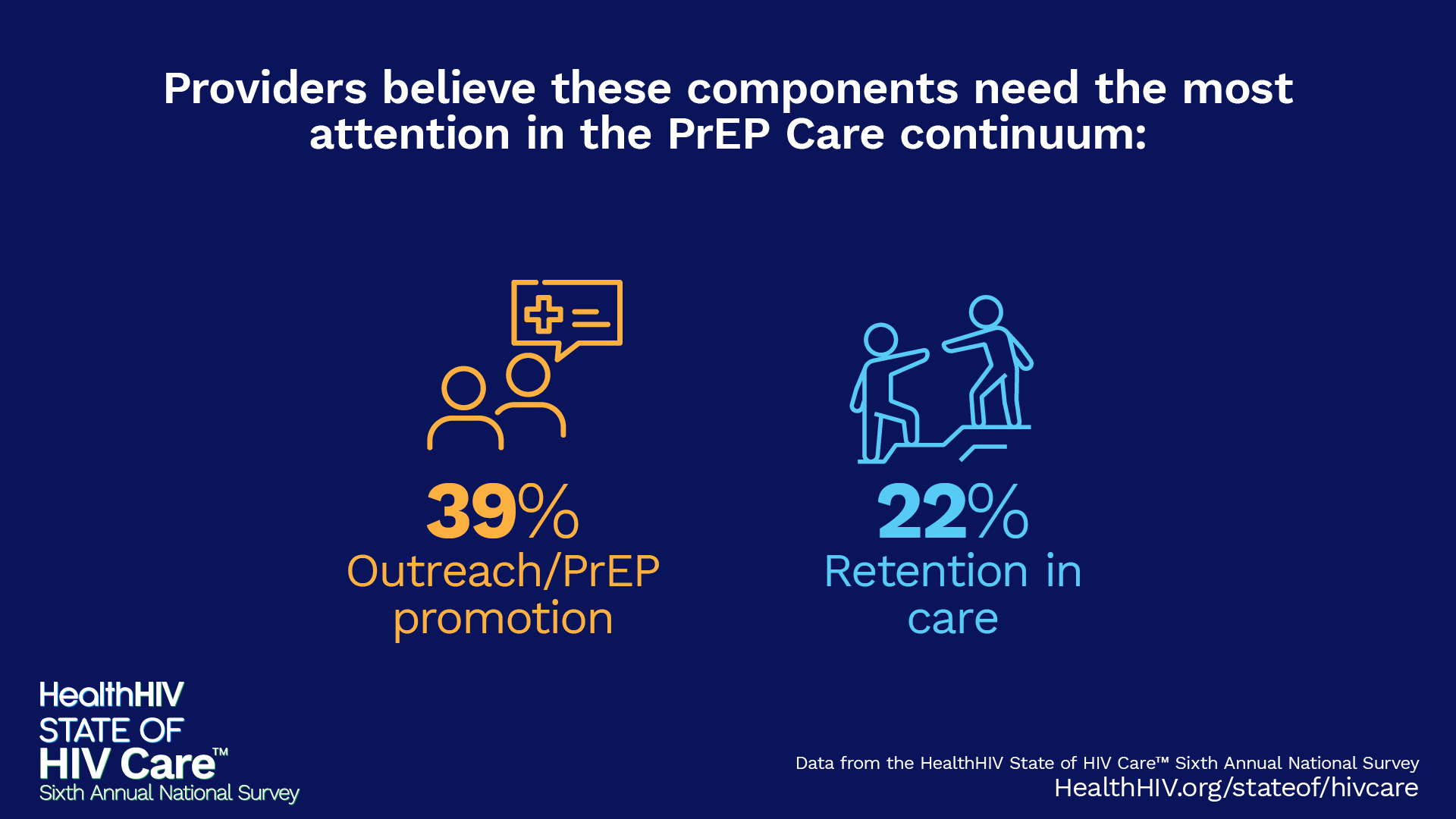
Download GraphicRetention in care is identified as the highest priority step in the HIV care continuum for the second year in a row. Increased retention and re-engagement in care will be necessary to meet EHE goals.
Providers believe these components need the most attention in the HIV Care continuum:
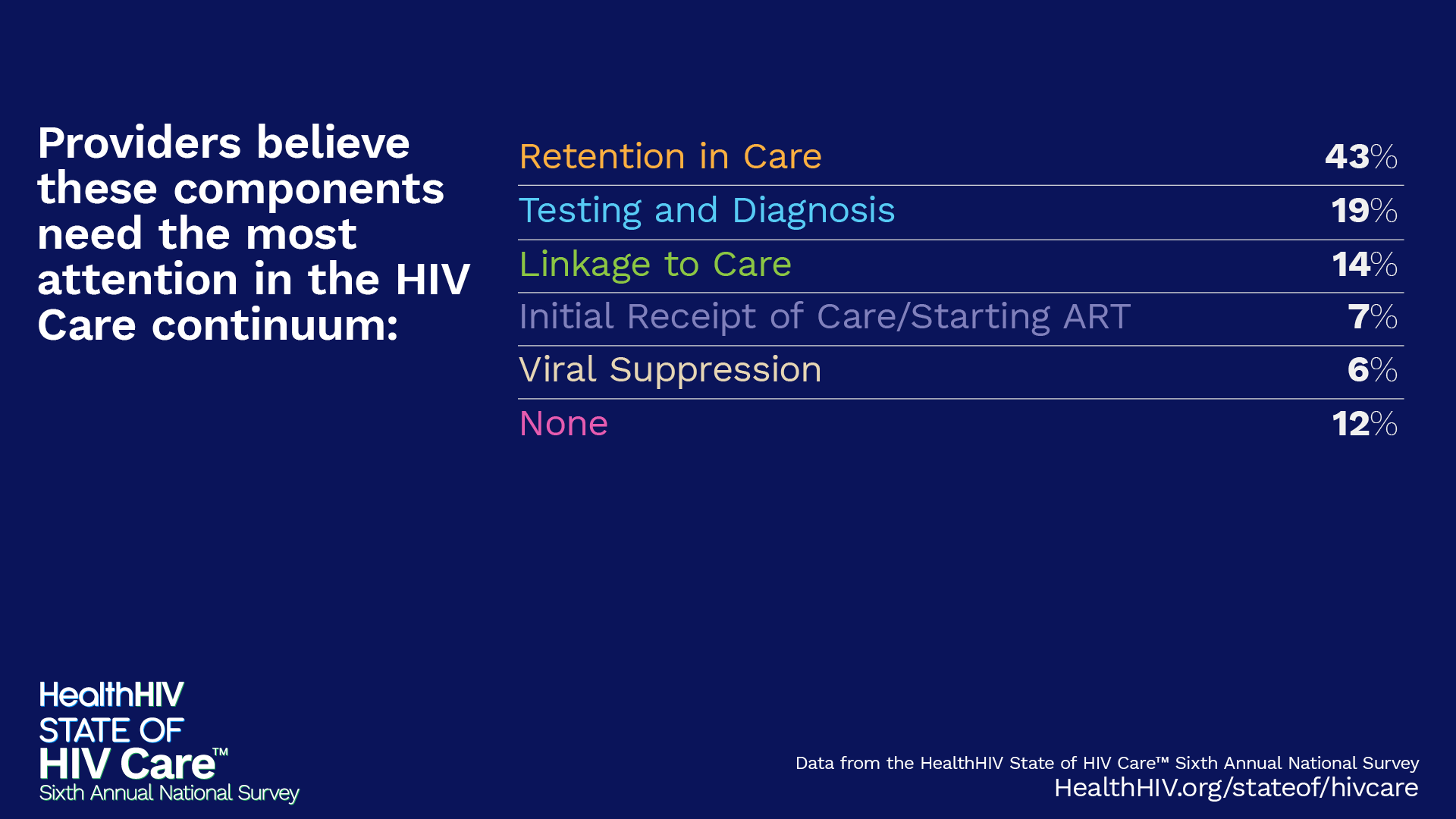 Download Graphic
Download GraphicSignificant engagement with long-acting injectables for HIV treatment suggests provider interest in novel approaches to care that might help their patients remain adherent to medication.7 However, it also suggests the need for training on and funding for other ways to support adherence, including virtual appointments, case management, and mobile services.
 Download Graphic
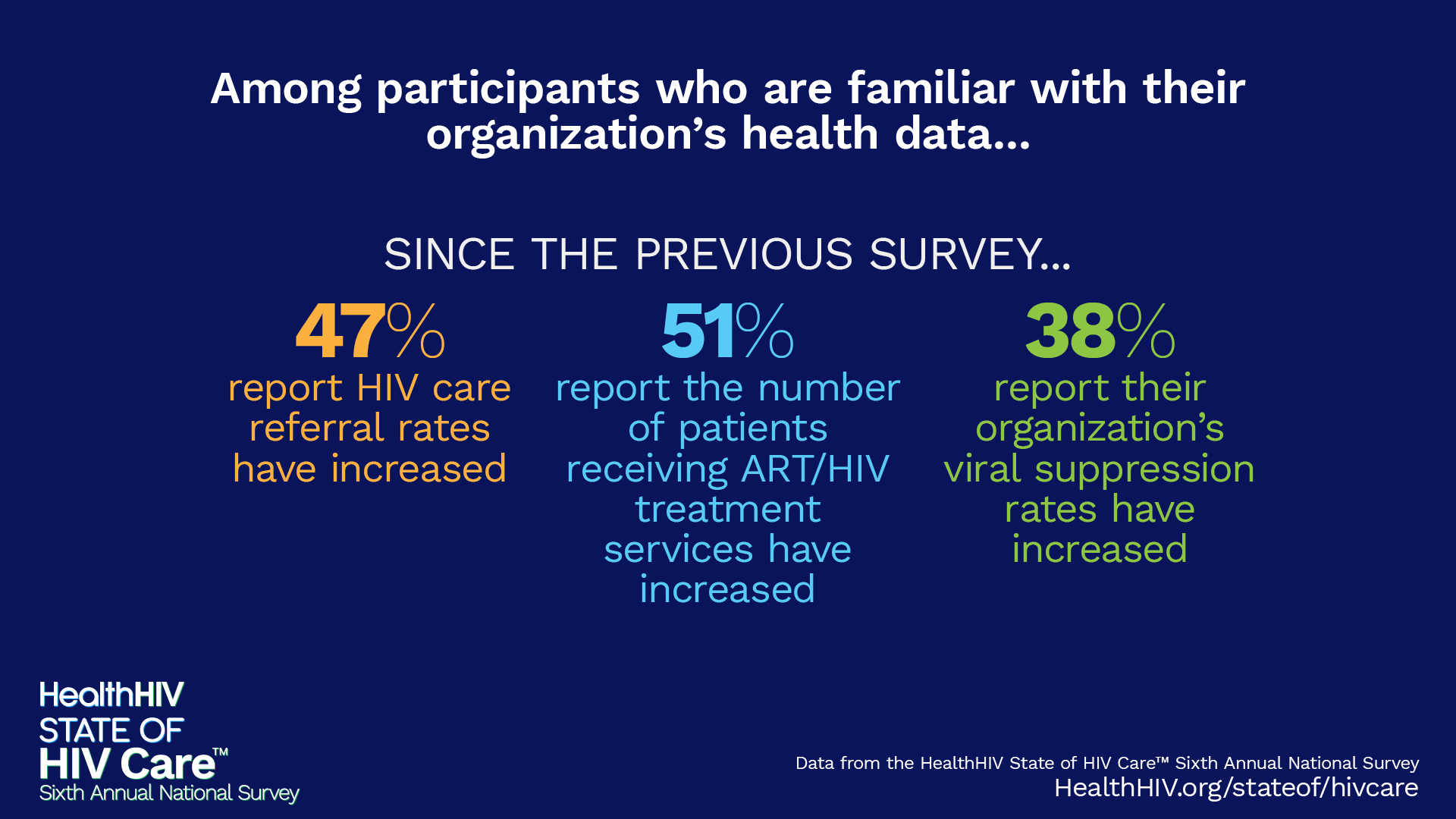
Download GraphicAmong participants who are familiar with their organization’s health data…
 Download Graphic
Download GraphicUrgent Need for Provider Training
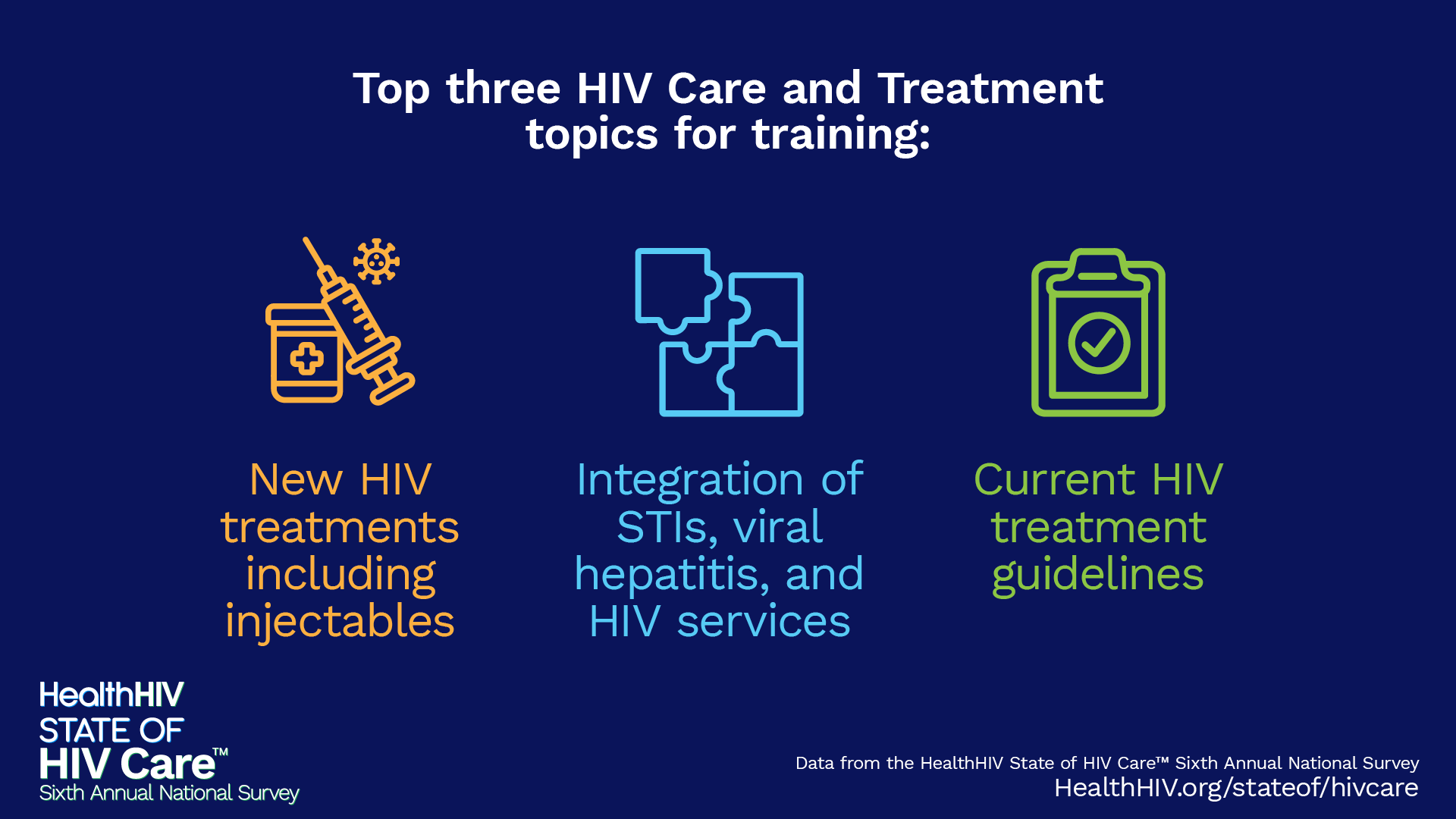
A growing demand among HIV care providers for training on treatment innovations and best practices is evident. This reflects the mounting pressures faced by the workforce to keep pace with rapid advancements in HIV care, as providers strive to meet the evolving needs of their patients in an increasingly complex healthcare landscape.
Top three HIV Care and Treatment topics for training:
 Download Graphic
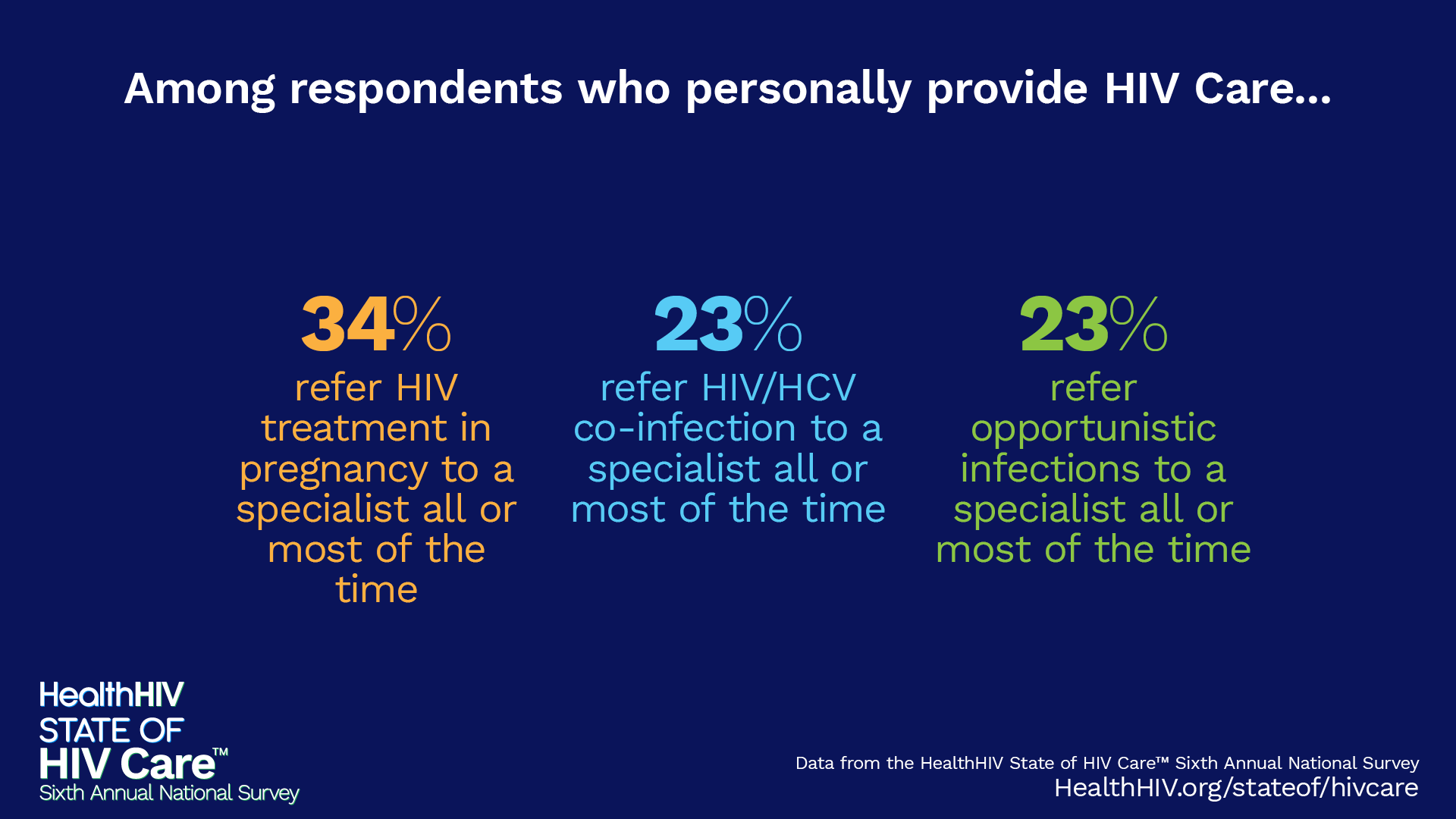
Download GraphicHIV treatment in pregnancy, HIV/HCV co-infection, and opportunistic infections represent several types of care that the average HIV care professional refers to specialists. These treatment concerns represent key areas for training. Increased confidence in treating complicated cases among non-specialist providers will contribute to greater care integration and efficiency.
Among respondents who personally provide HIV care…
 Download Graphic
Download GraphicHurdles in HIV Treatment Access
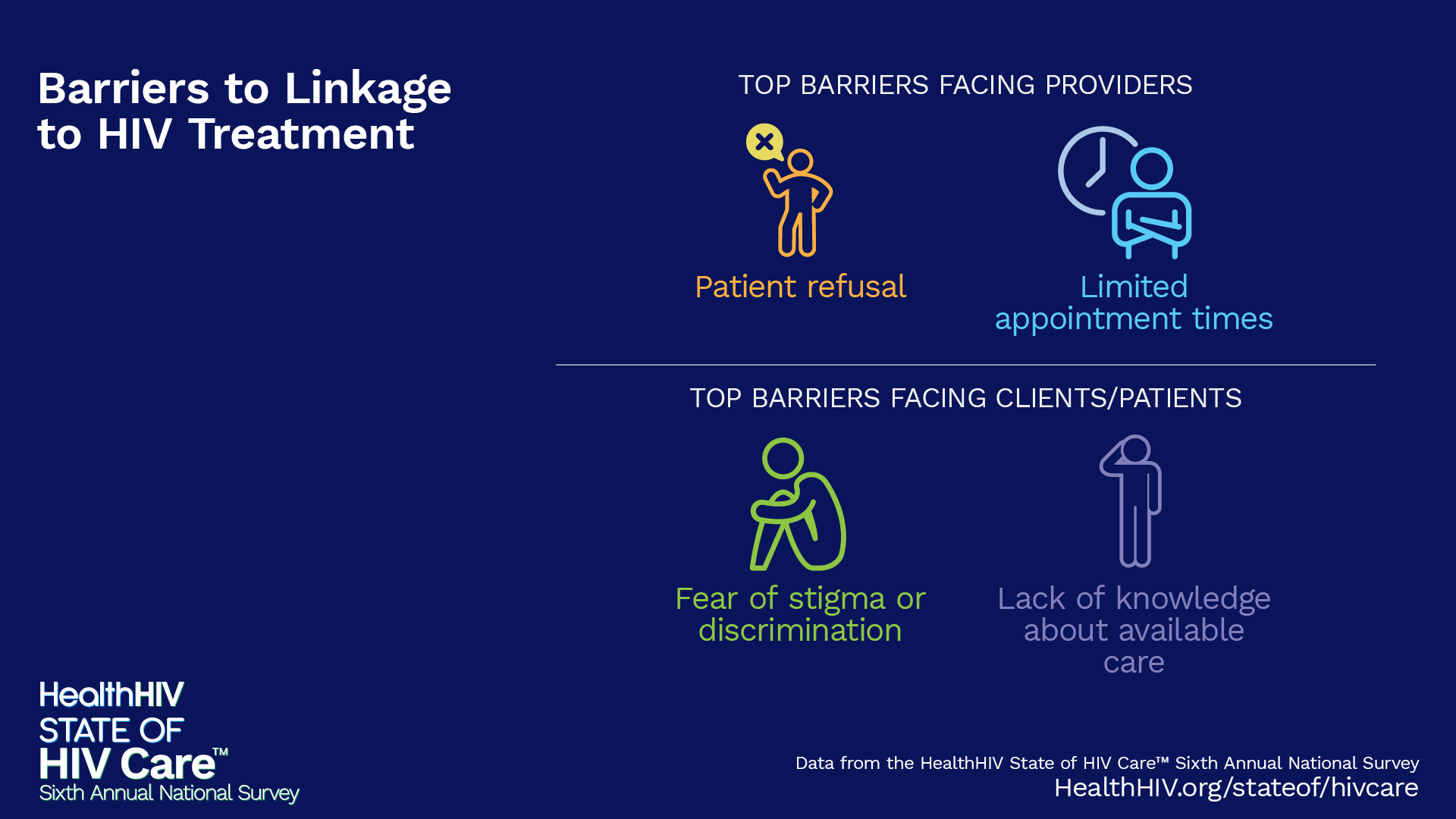
Providers often face patient refusals when attempting to link individuals to HIV treatment following diagnosis. Even when patients are willing, the struggle to secure timely appointments persists. These barriers underscore the urgent need for an expanded workforce and the adoption of alternative care models, such as pharmacist-led or mobile device-based treatment, to better serve diverse populations and improve access to care.8, 9
Linkage to Care
 Download Graphic
Download GraphicStarting ART
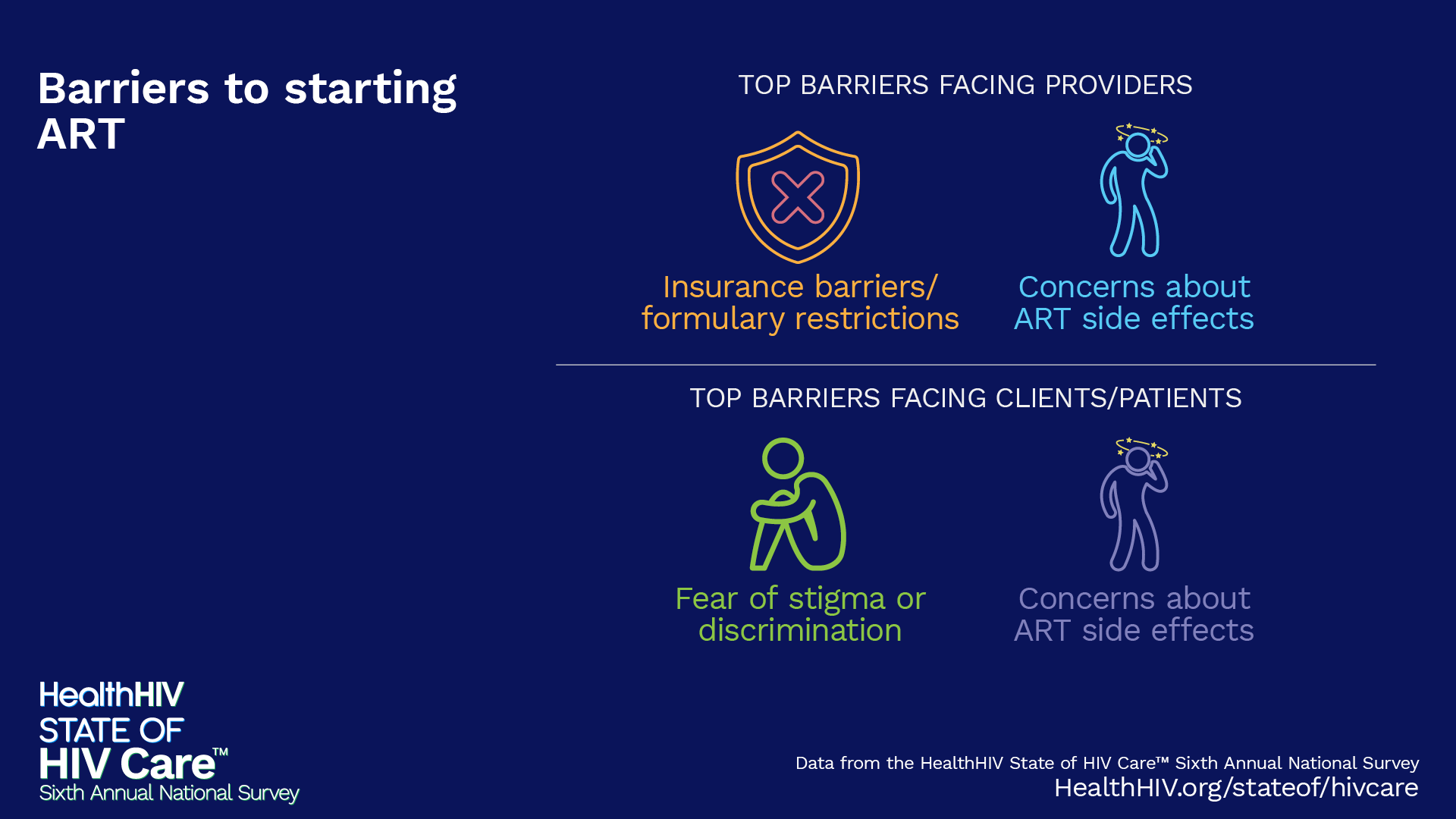
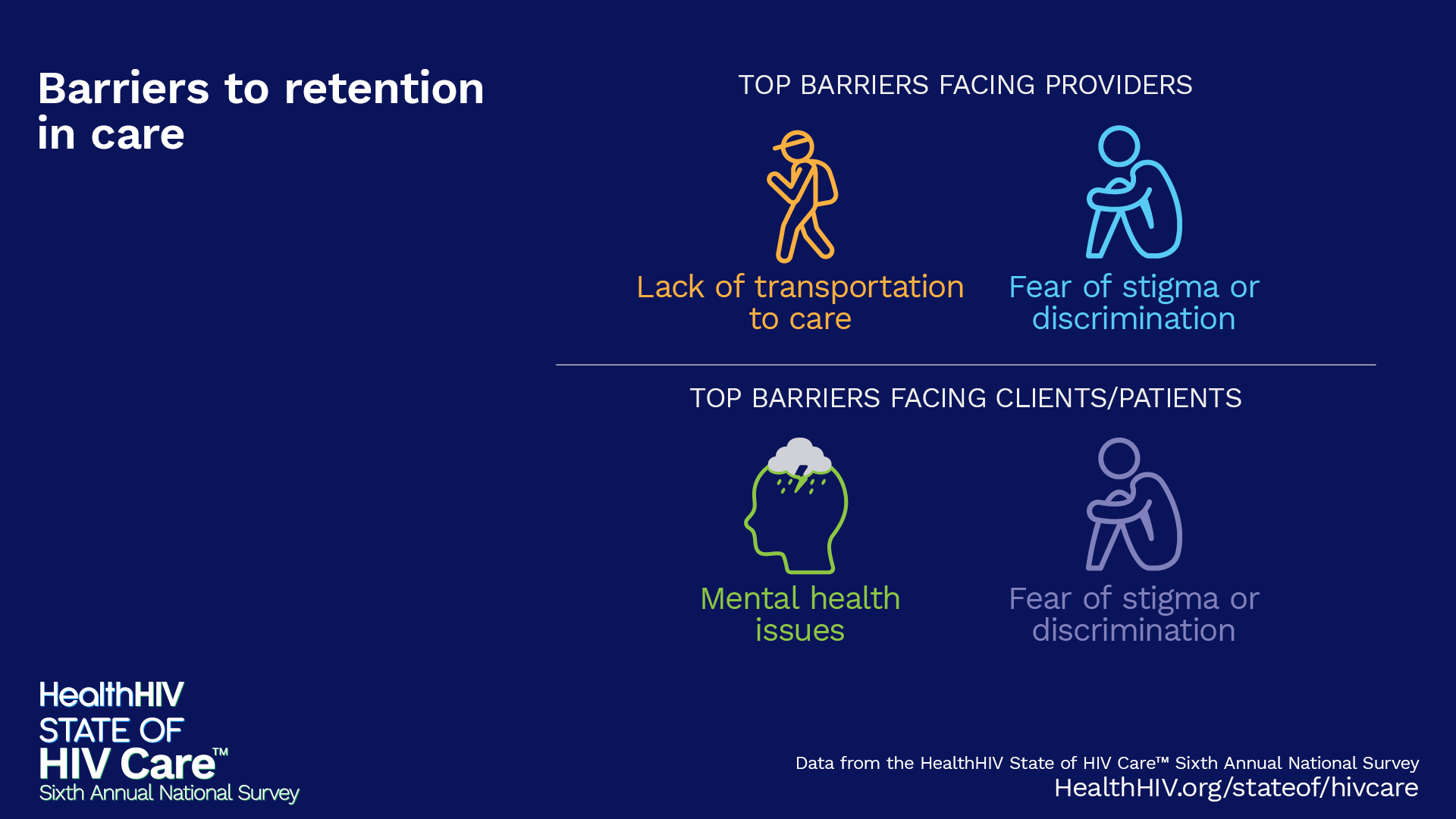
Once patients are linked to treatment, insurance barriers often disrupt smooth ART initiation, a process that may be further complicated by patient concern about medication side effects. Even more, social barriers like transportation instability and stigma prevent many from staying in care once treatment has been initiated.
 Download Graphic
Download GraphicRetention in Care
 Download Graphic
Download GraphicInsurance Barriers
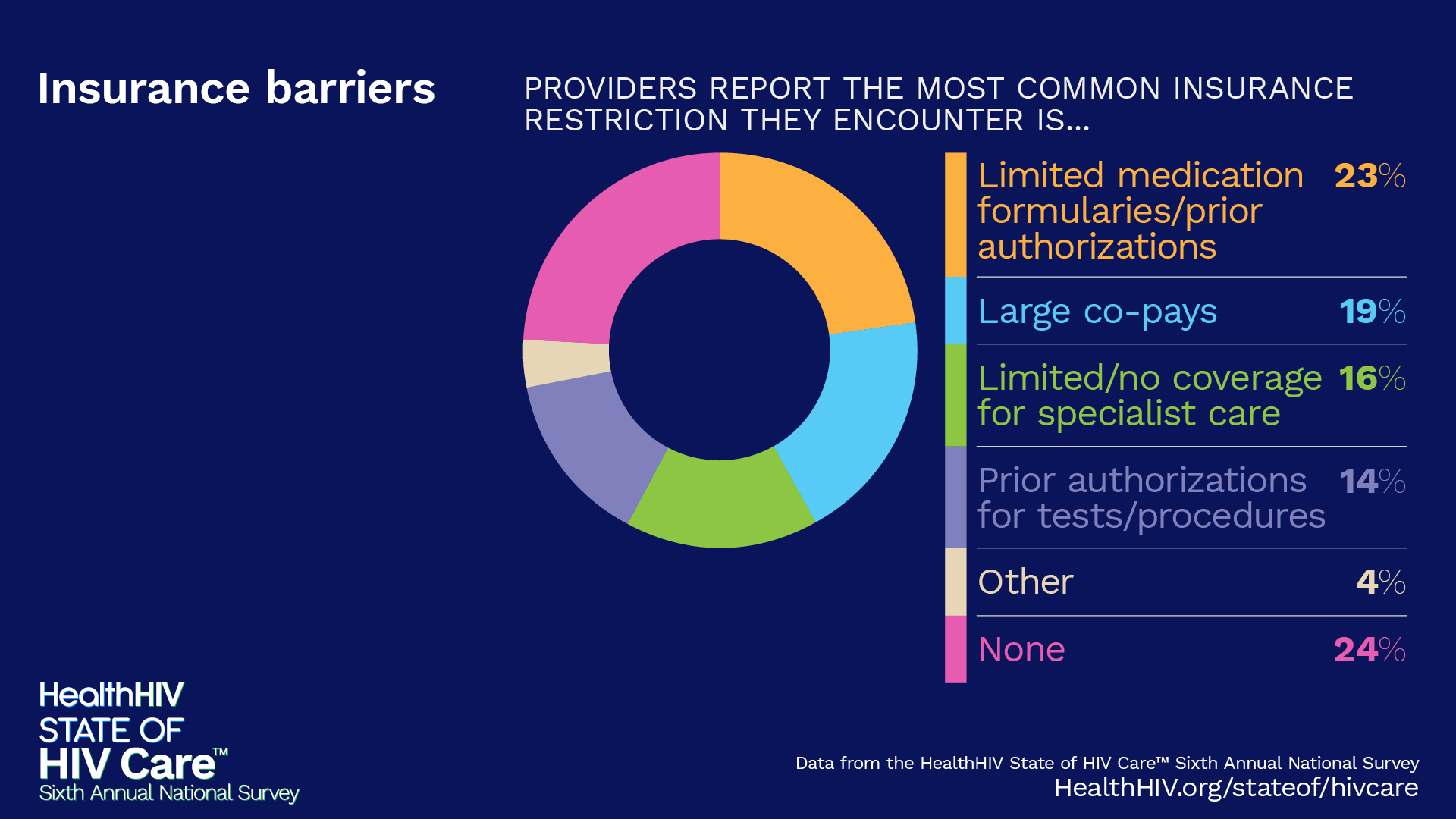
Insurance issues can create significant barriers to timely care. Providers are often prevented from offering crucial services due to payer restrictions including prior authorization requirements, large co-pays, and limited formularies.
- Providers report private employer-sponsored insurance generally requires the most time to complete and receive a determination for ART.
- 29% of respondents report being unable to provide HIV services due to payer/insurance restrictions sometimes, often, or all the time.
 Download Graphic
Download GraphicProviders believe these components need the most attention in the PrEP Care continuum:
 Download Graphic
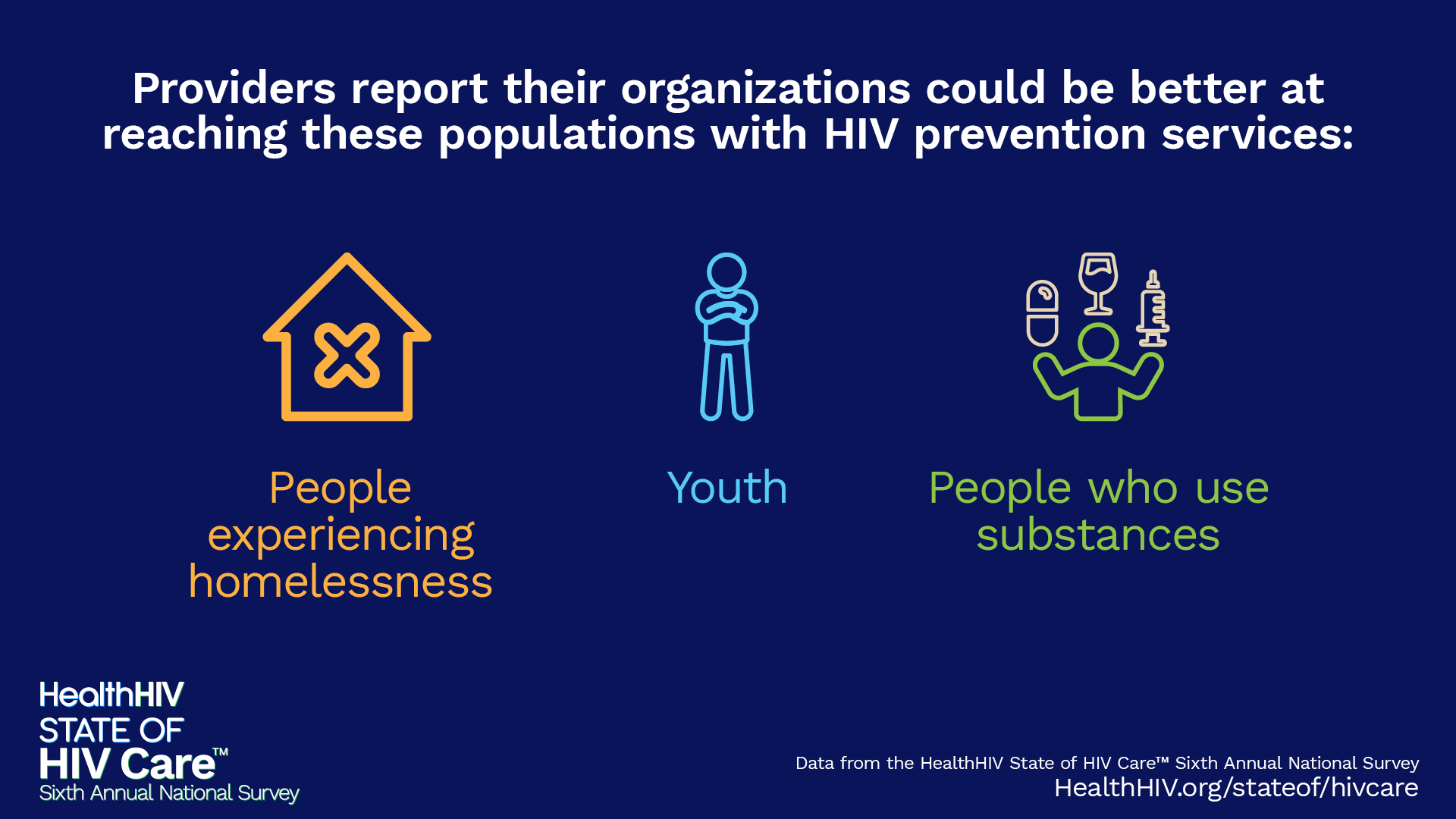
Download GraphicProviders report their organizations could be better at reaching these populations with HIV prevention services:
 Download Graphic
Download GraphicThe majority of participants familiar with their organization’s health data report testing and PrEP usage rates have increased over the last year. However, increased funding and workforce preparation are needed to maintain upward trends.
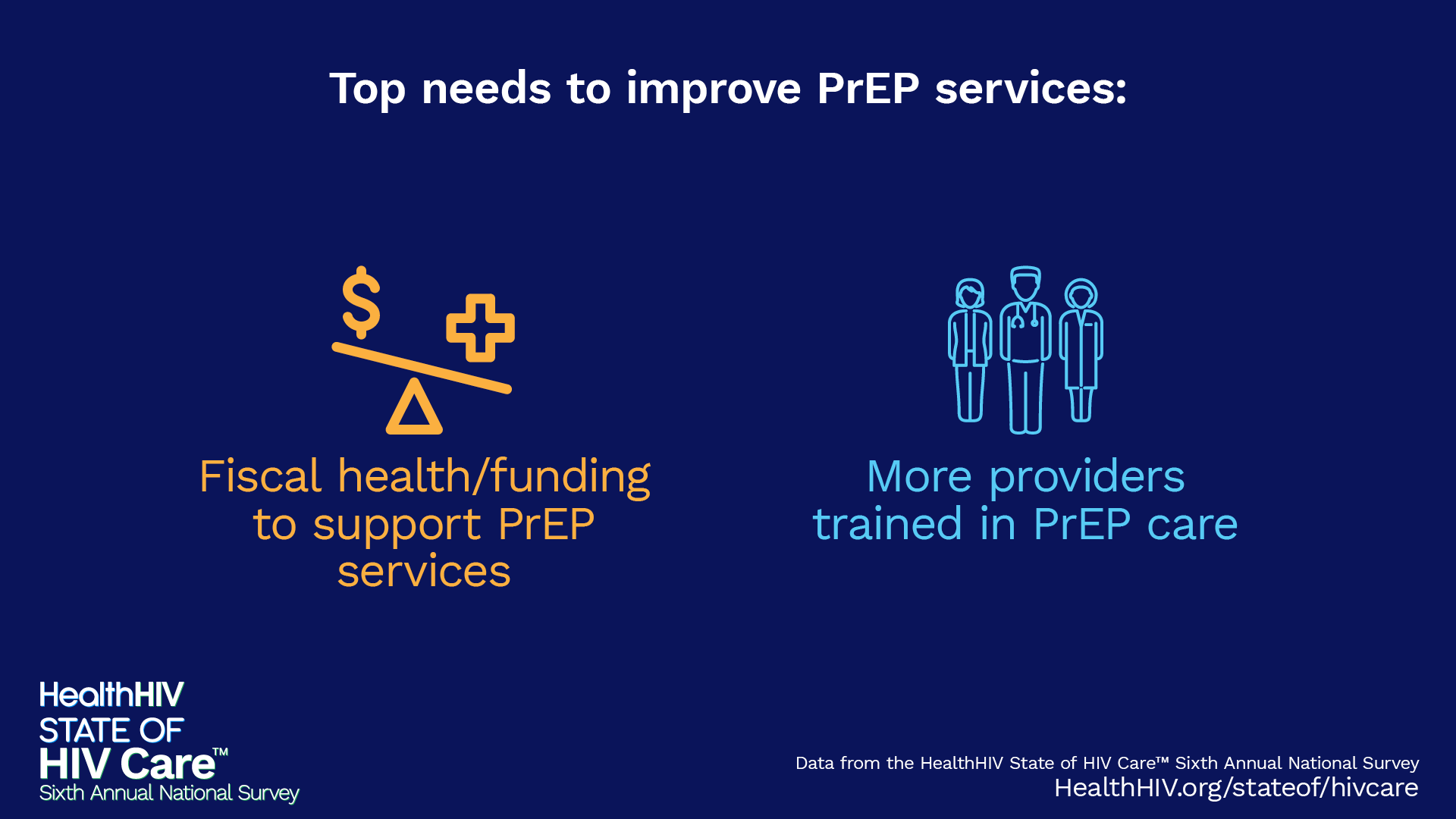
Top needs to improve PrEP services:
 Download Graphic
Download GraphicAmong participants who are familiar with their organization’s health data…
 Download Graphic
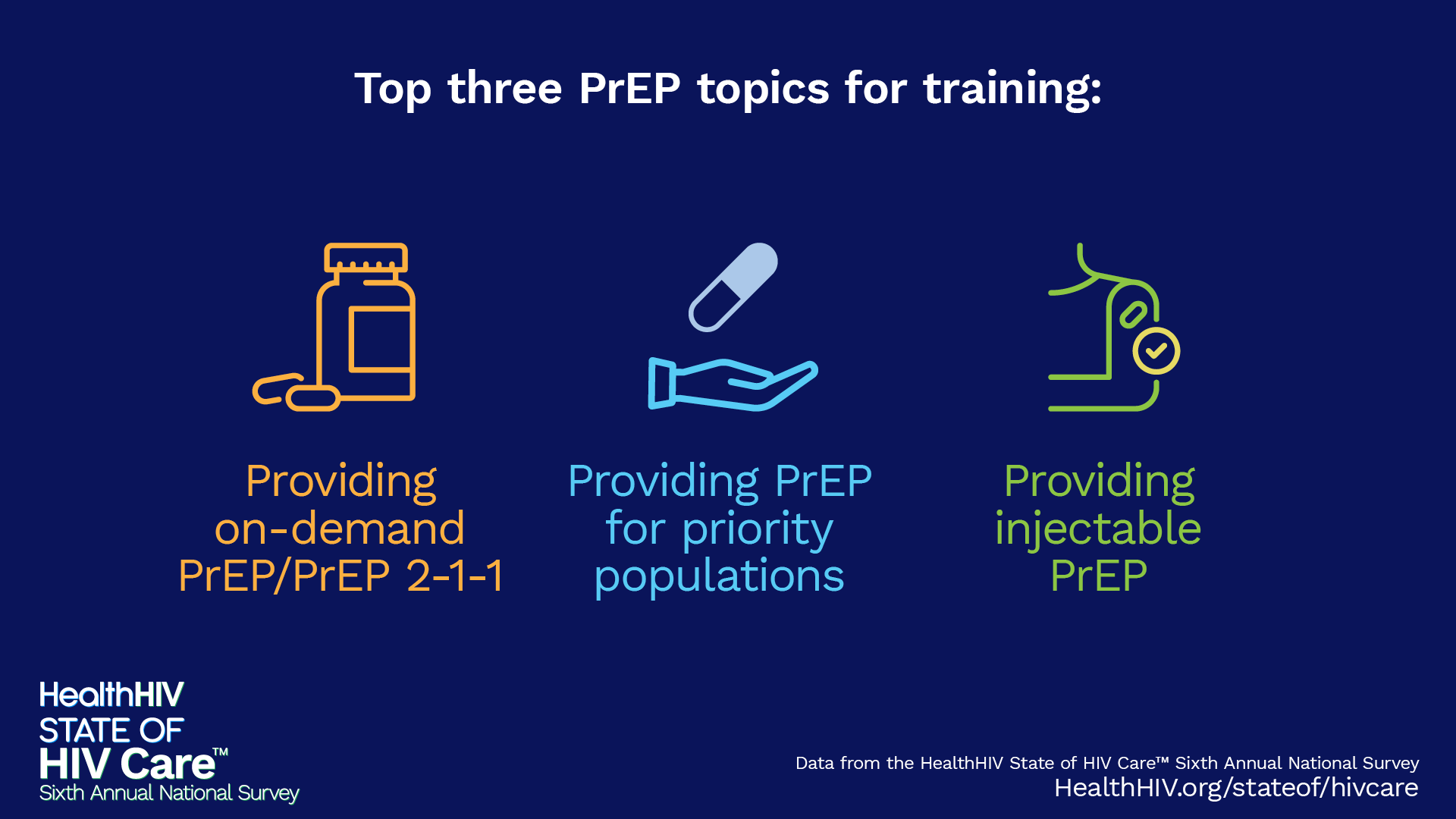
Download GraphicTraining and Knowledge Gaps in PrEP Care
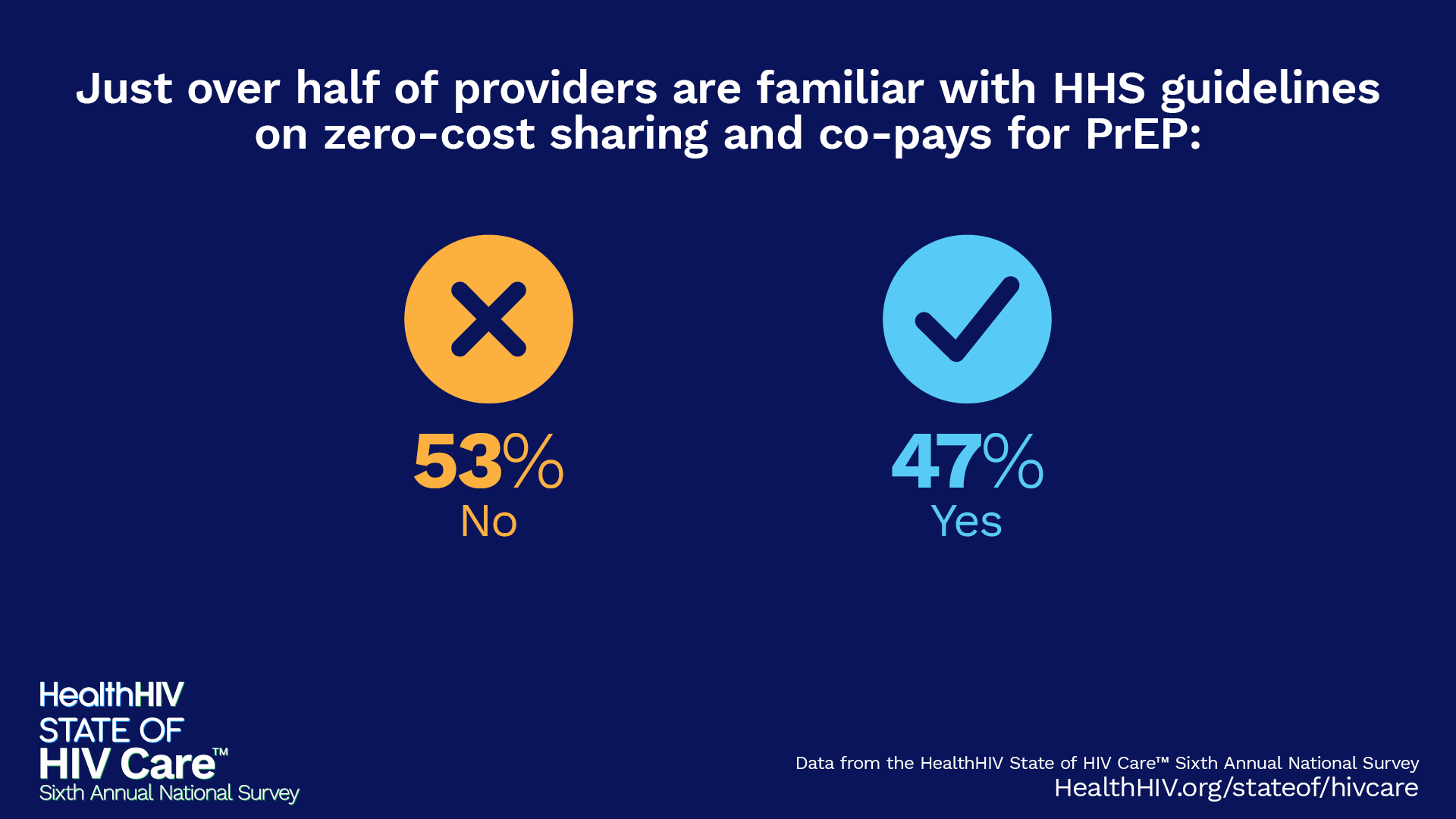
PrEP providers are seeking more training on emerging prevention innovations, such as on-demand PrEP and injectables, as well as on how to provide PrEP to priority populations. Additionally, less than half of respondents are familiar with the Department of Health and Human Services guidelines on zero-cost sharing and co-pays for PrEP, indicating a significant gap in provider knowledge that needs to be addressed.
Top three PrEP topics for training:
 Download Graphic
Download GraphicJust over half of providers are familiar with HHS guidelines on zero-cost sharing and co-pays for PrEP:
 Download Graphic
Download GraphicCritical Barriers to Prevention Exposed
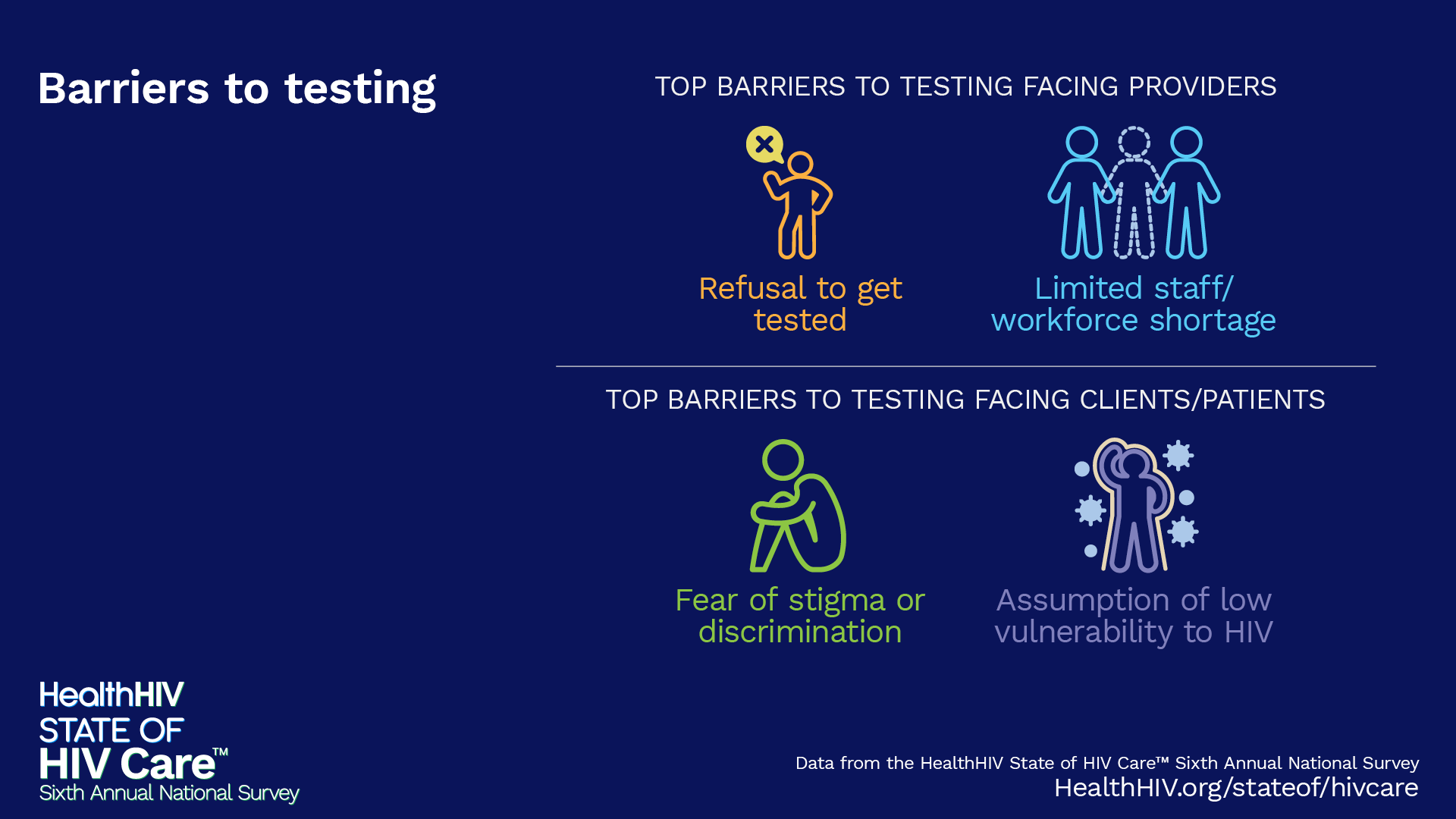
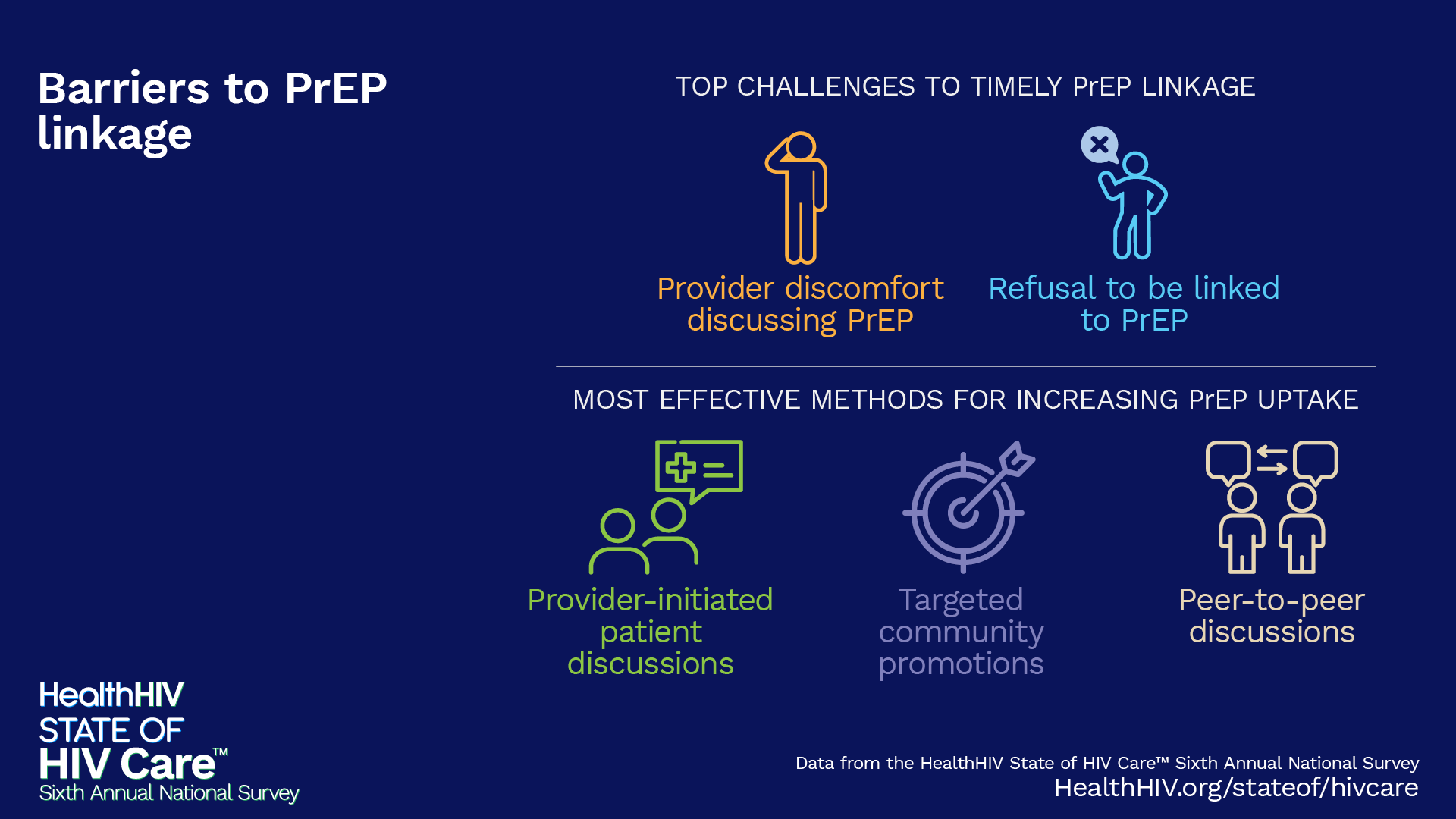
Patient refusal, fueled by stigma or a false sense of invulnerability to HIV, stands as a major barrier to both HIV testing and PrEP linkage. Providers also cite workforce shortages and discomfort discussing PrEP as significant obstacles. Even once patients are linked to care, insurance restrictions emerge as the greatest hurdle to prescribing PrEP, underscoring the complex challenges in delivering effective prevention.
Testing
 Download Graphic
Download GraphicLinking to PrEP
 Download Graphic
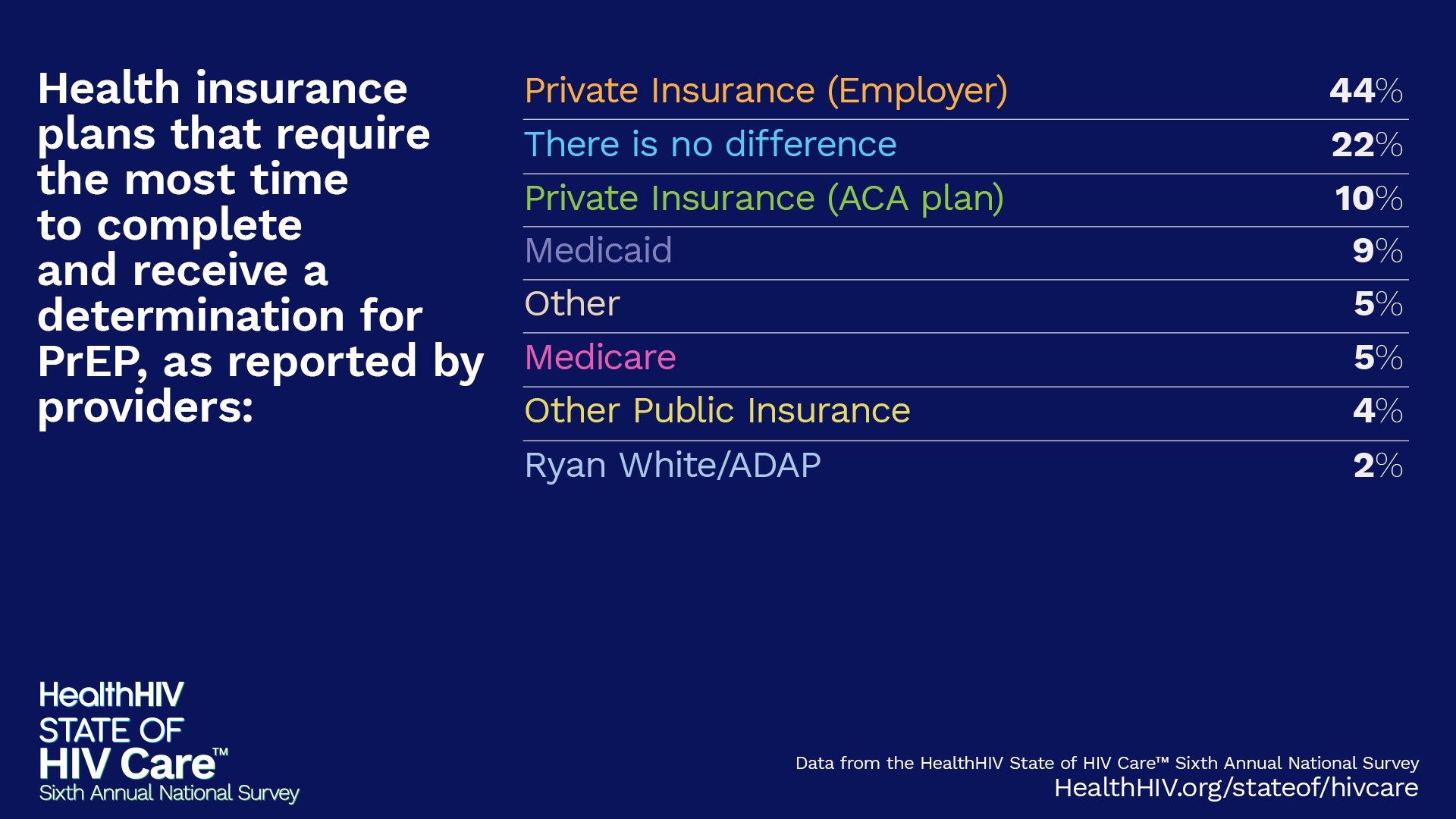
Download GraphicHealth insurance plans that require the most time to complete and receive a determination for PrEP, as reported by providers:
 Download Graphic
Download GraphicPrescribing PrEP
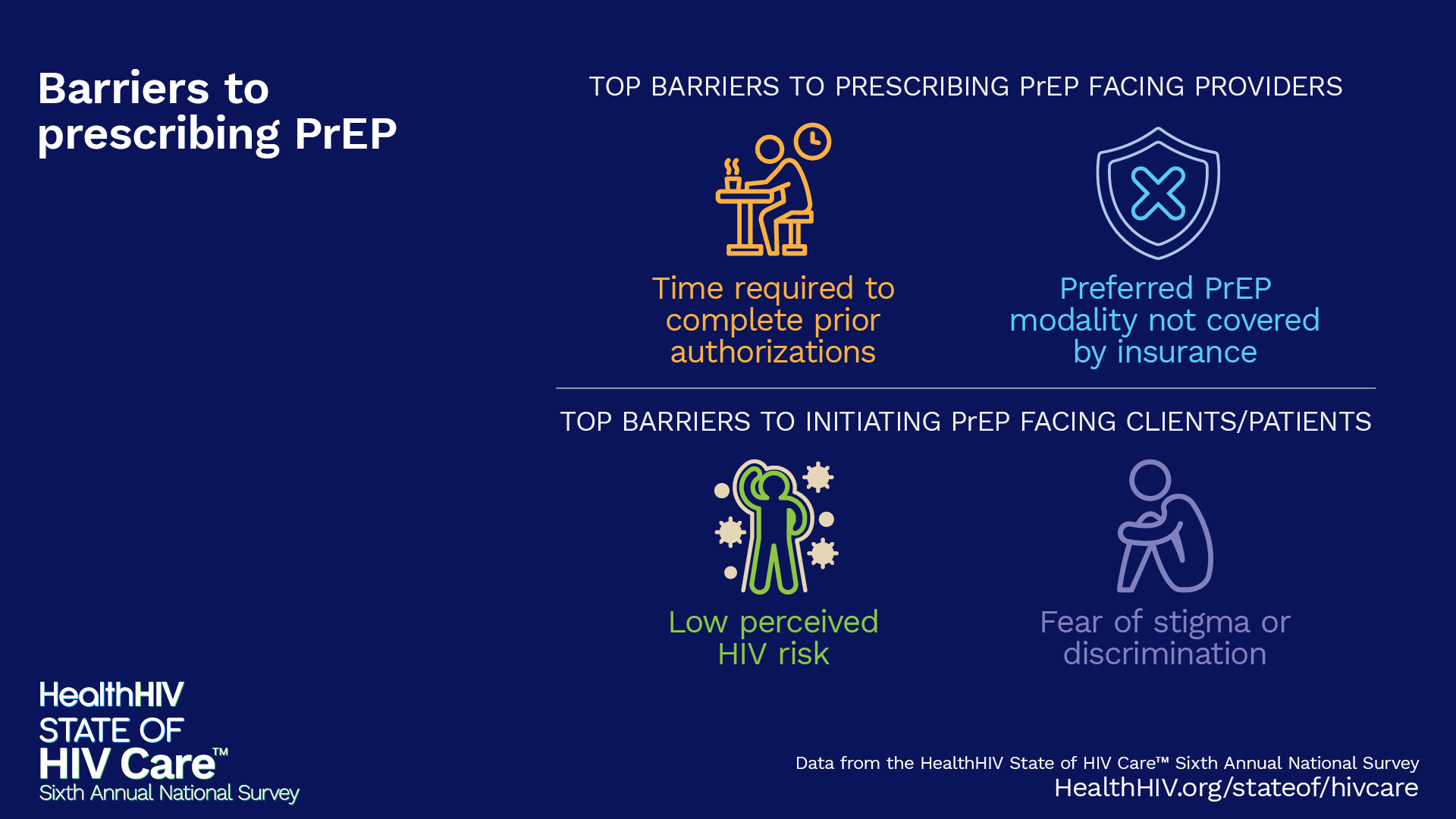 Download Graphic
Download GraphicMost common reasons clients/patients discontinue PrEP:
 Download Graphic
Download GraphicMost respondents believe there are not enough behavioral health providers to meet the demand for services:
 Download Graphic
Download GraphicBarriers to Behavioral Health Care for People with HIV
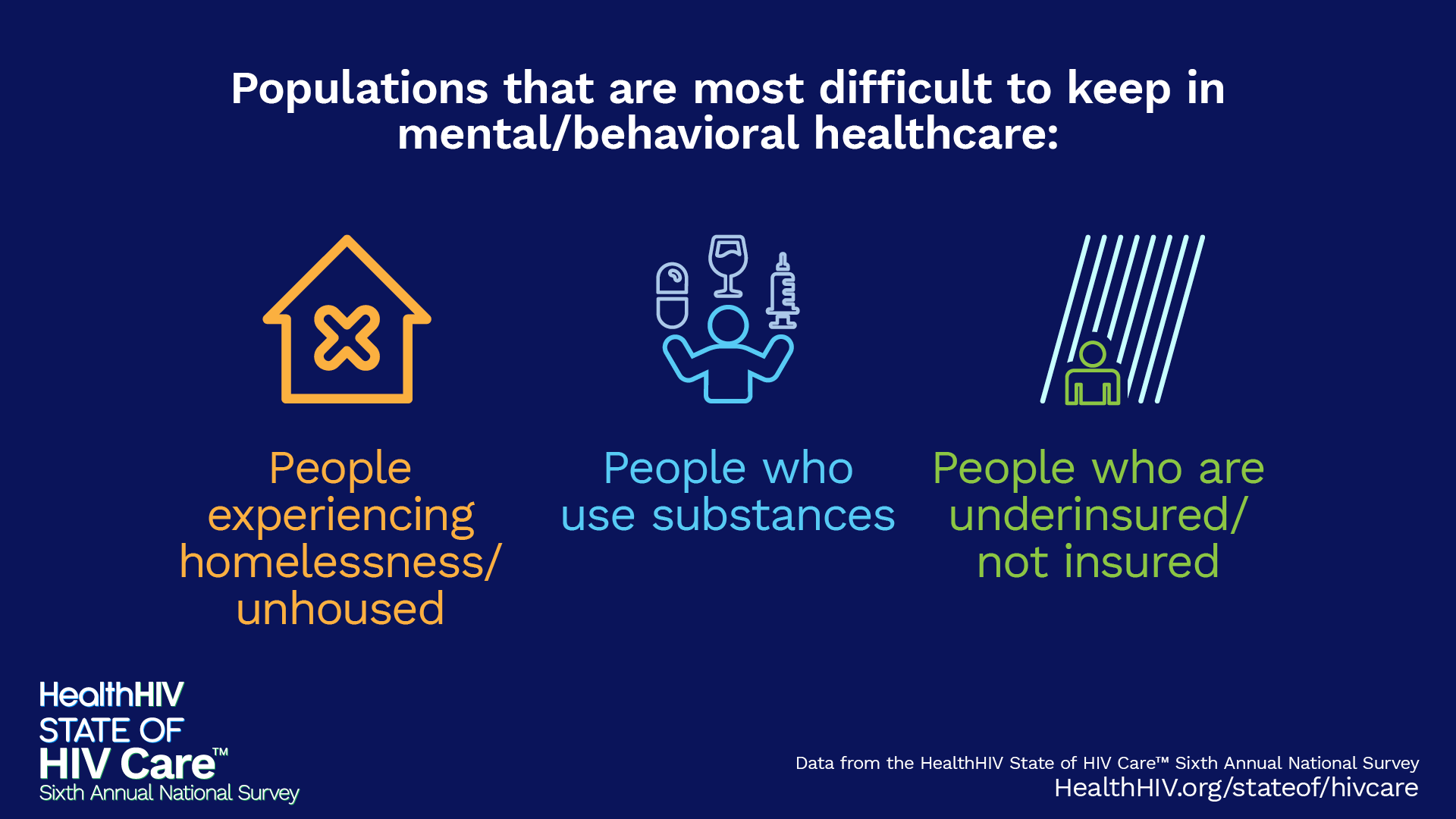
Fear of stigma or discrimination, along with a lack of trust in health systems and professionals, are major challenges to accessing mental health services for people with HIV (PWH). Providers report that retaining patients in mental and behavioral healthcare is particularly difficult for populations such as those experiencing homelessness, people who use substances, and individuals who are underinsured or uninsured. These barriers highlight critical gaps in care for priority populations.
Top challenges to accessing mental health services from the patient/client perspective:
 Download Graphic
Download GraphicPopulations that are most difficult to keep in mental/behavioral healthcare:
 Download Graphic
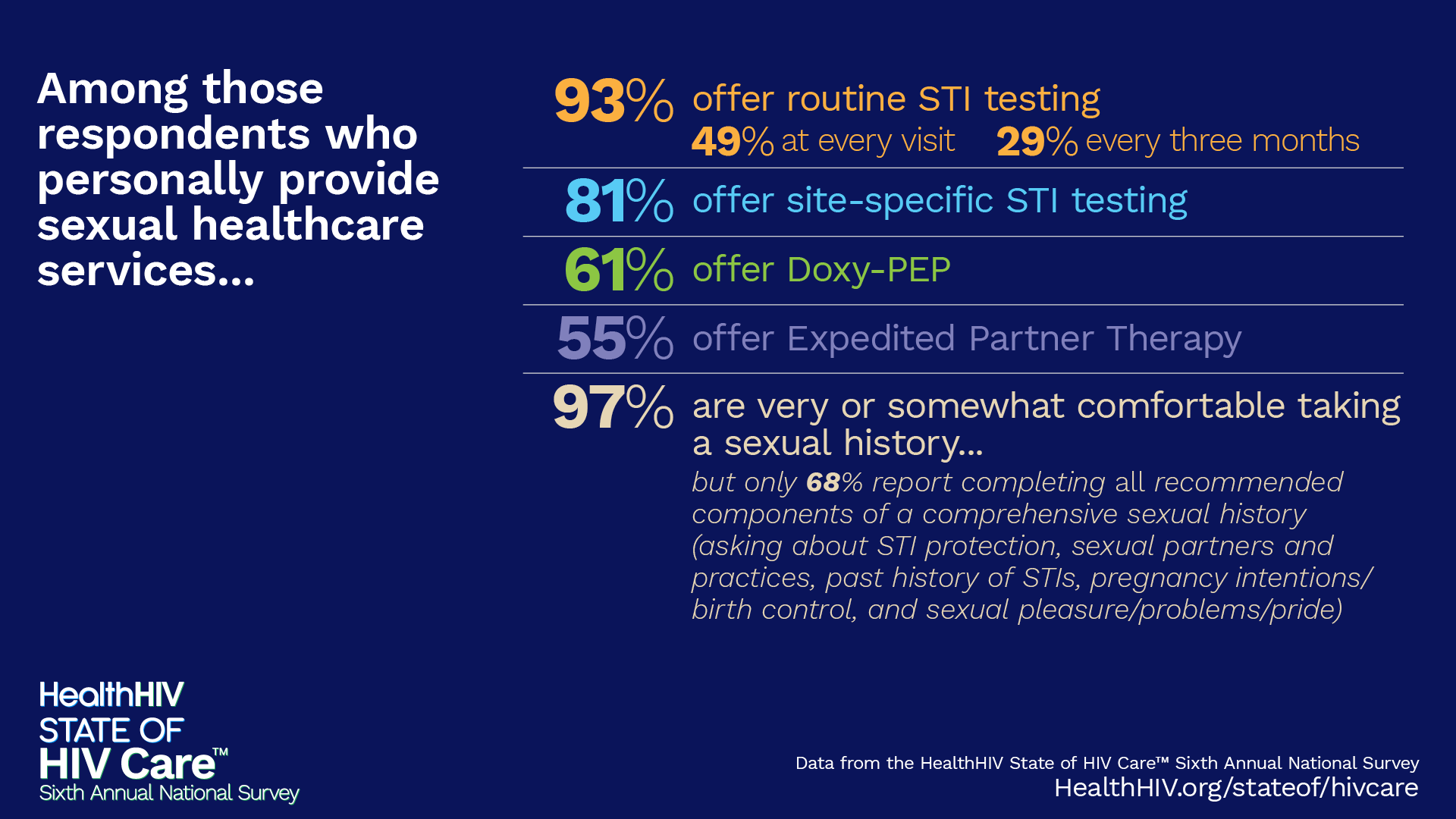
Download GraphicBest Practices for Sexual Healthcare
Among those respondents who personally provide sexual healthcare services…
 Download Graphic
Download GraphicThe majority of providers believe HIV criminalization policies impact the health of their clients:
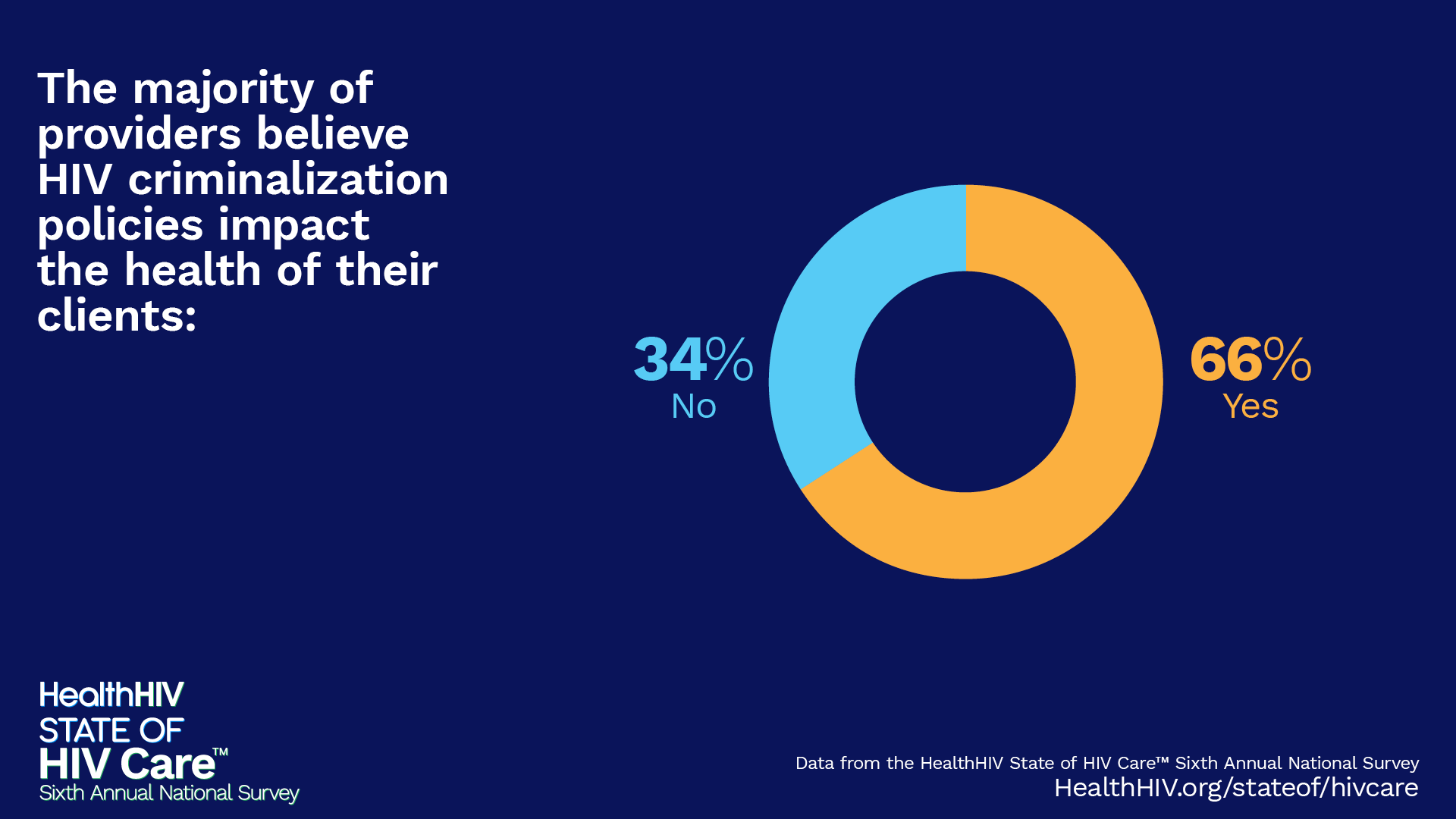 Download Graphic
Download GraphicThe majority of providers believe that HIV criminalization policies have a negative impact on public health efforts to prevent HIV transmission:
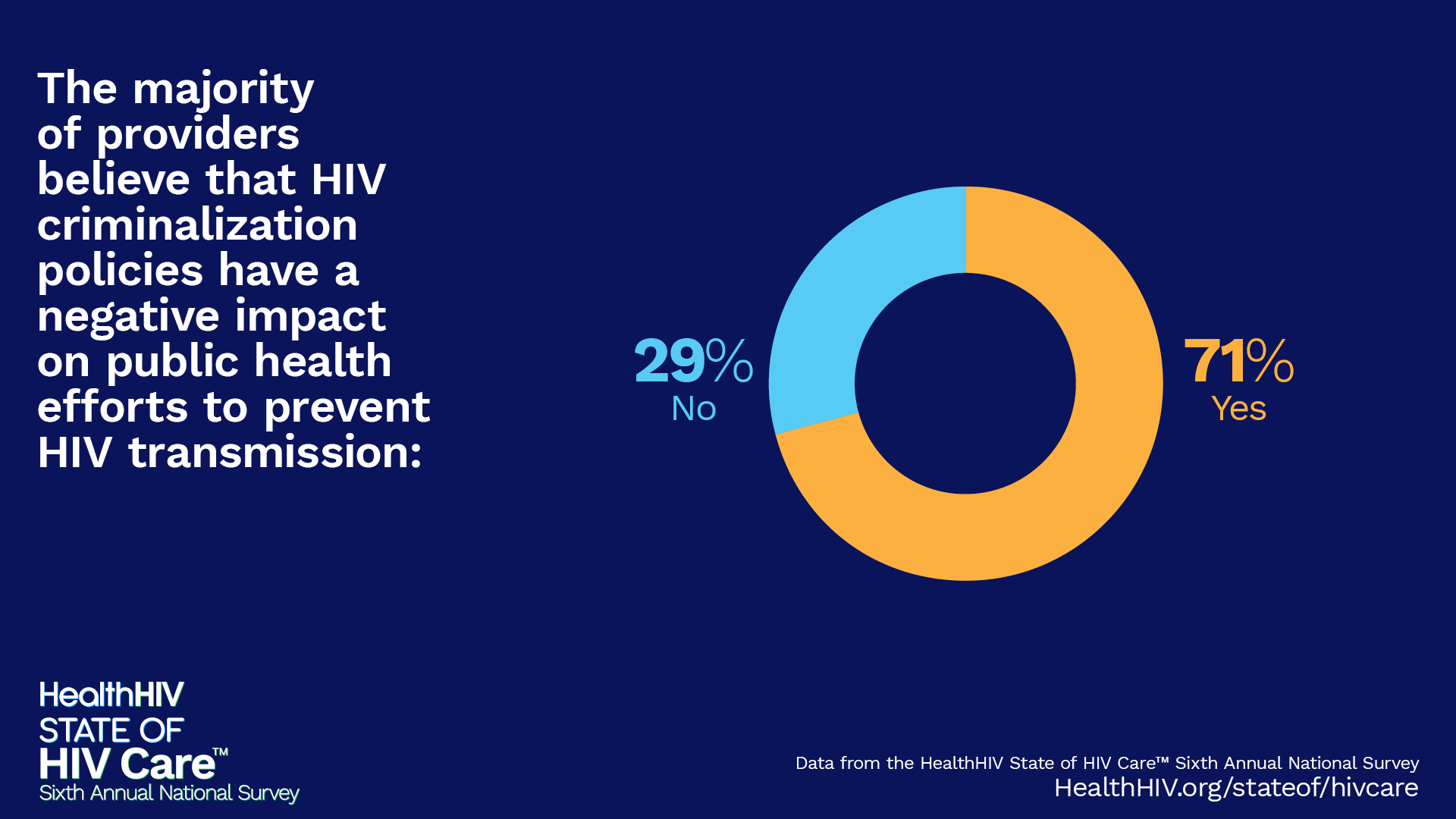 Download Graphic
Download GraphicMost providers have never counseled a patient on legal risks related to HIV criminalization:
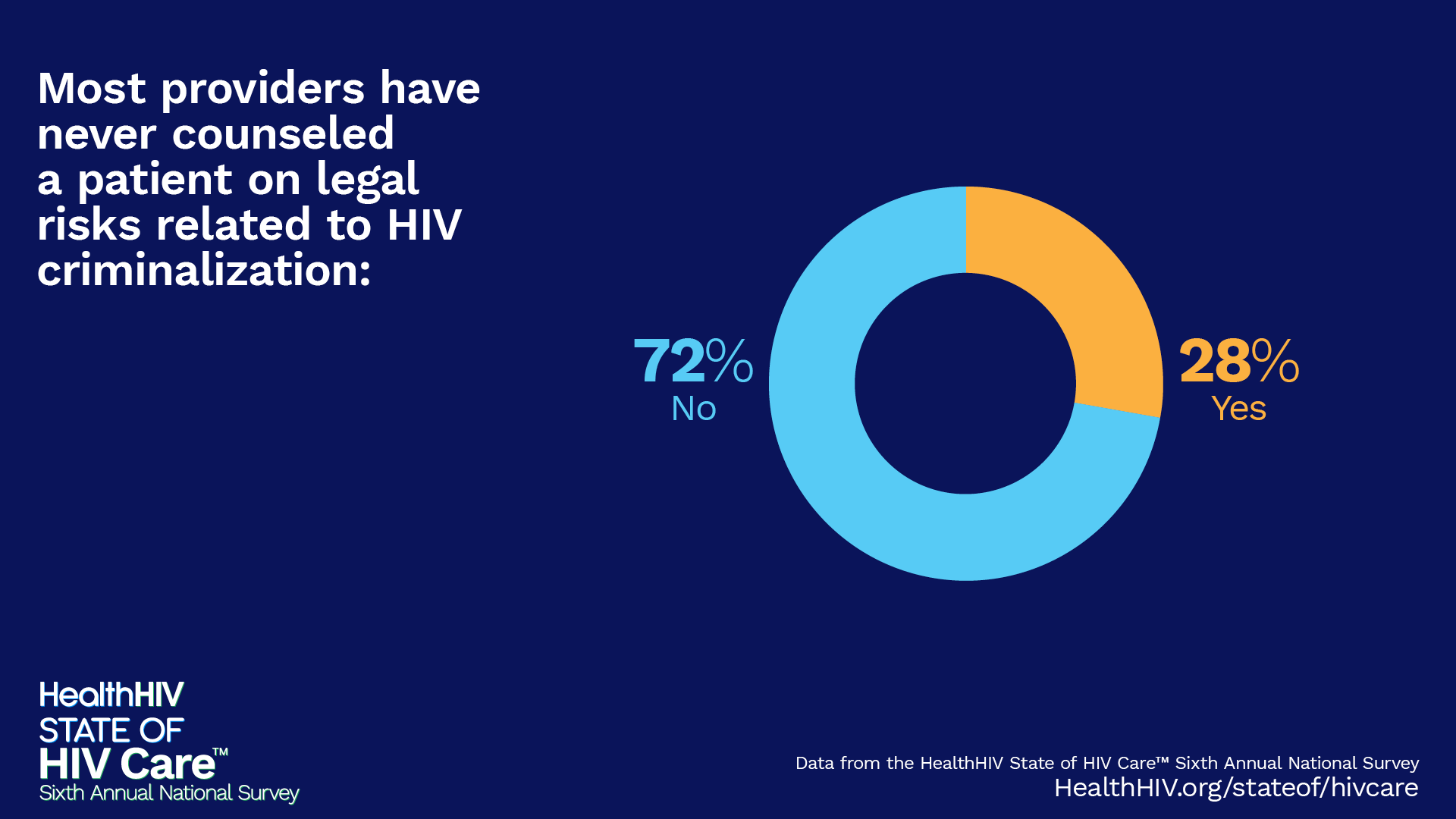 Download Graphic
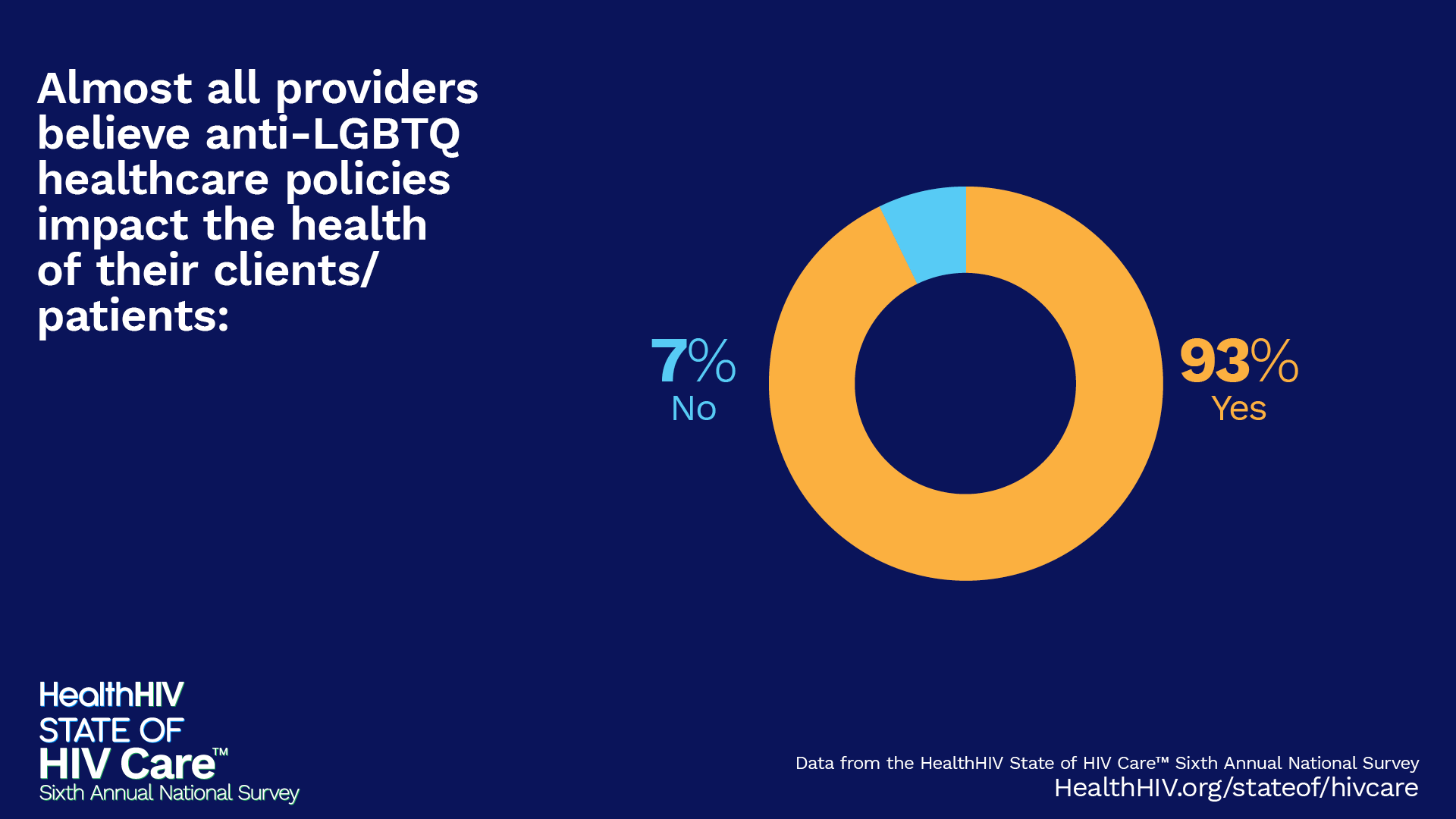
Download GraphicAlmost all providers believe anti-LGBTQ healthcare policies impact the health of their clients/patients:
 Download Graphic
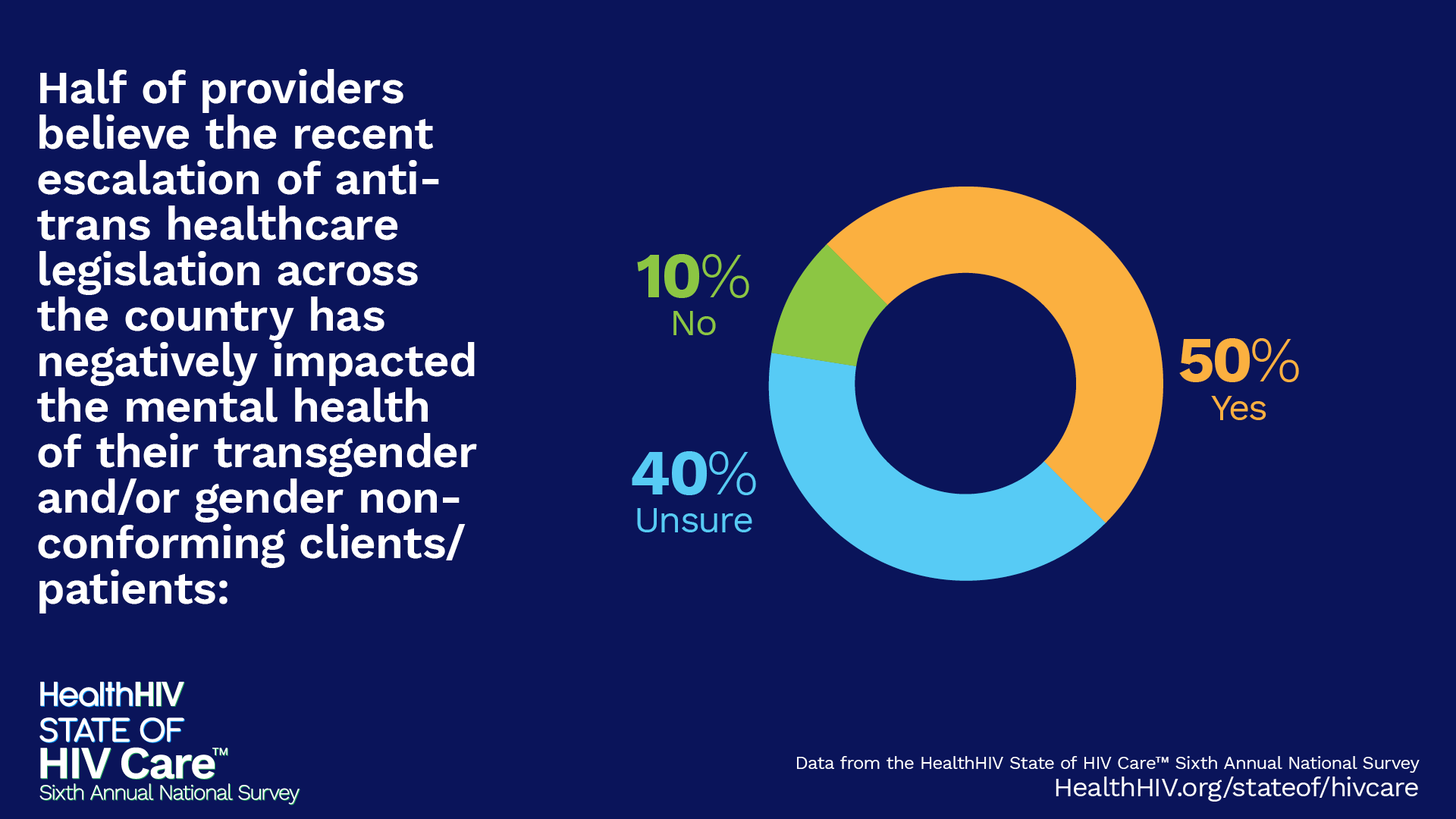
Download GraphicHalf of providers believe the recent escalation of anti-trans healthcare legislation across the country has negatively impacted the mental health of their transgender and/or gender non-conforming clients/patients:
 Download Graphic
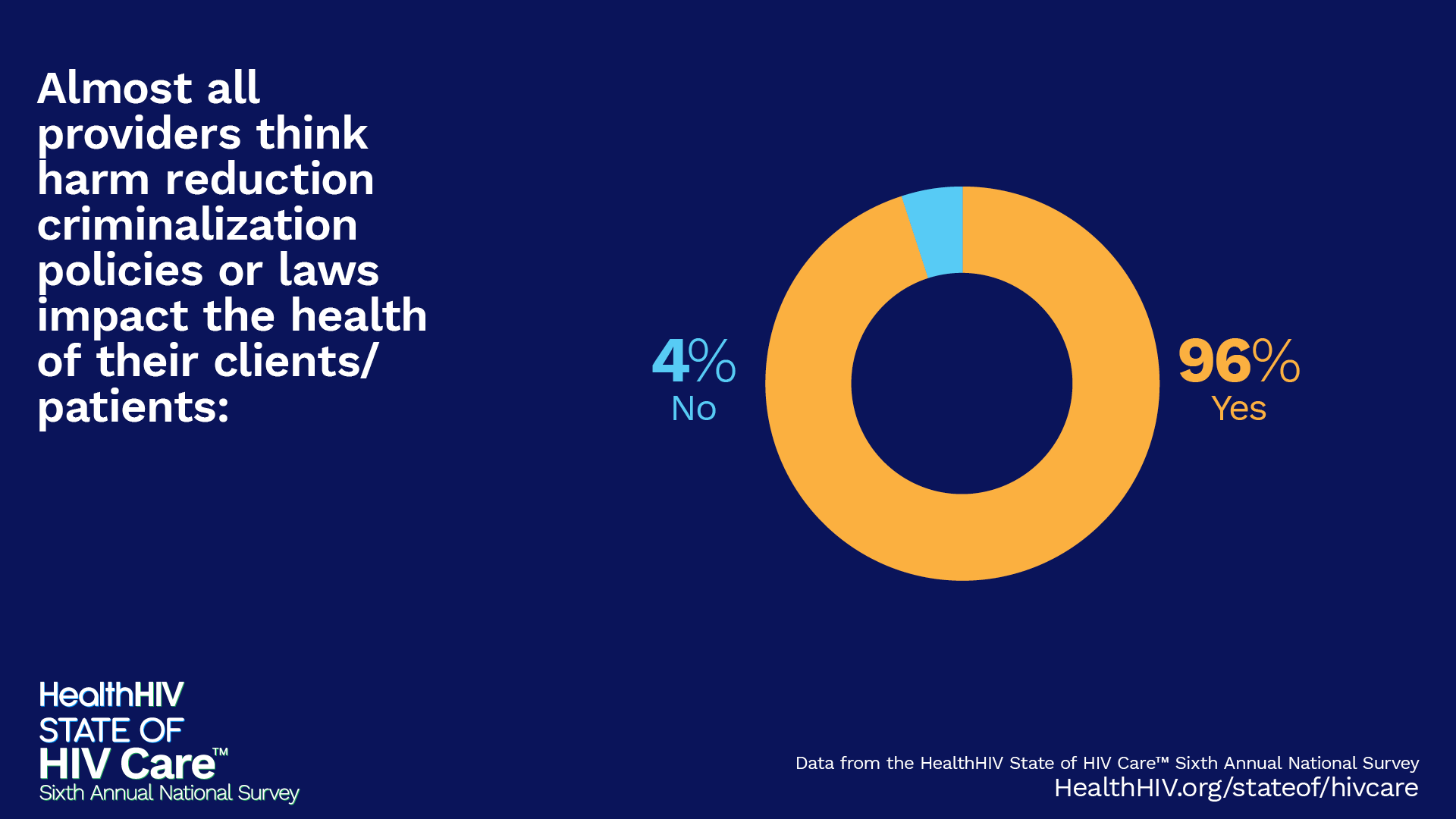
Download GraphicAlmost all providers think harm reduction criminalization policies or laws impact the health of their clients/patients:
 Download Graphic
Download GraphicImplications and Opportunities
The survey findings highlight the complex disconnect between barriers and opportunities to optimize HIV care and end the epidemic.
Barrier
The current HIV workforce is facing significant challenges, with experienced providers reporting burnout, poor compensation, and an approaching wave of retirements.18 While the gap between available, trained HIV providers and PWH grows, we have entered the next phase in HIV treatment development that has the opportunity to end the epidemic. In order to capitalize on new therapy development and true HIV care innovation, an expanded and experienced workforce is needed.
Opportunity
Expanding training opportunities for the next generation of HIV care providers, including primary care and general medicine professionals, can help alleviate workforce shortages and burnout. The survey demonstrated providers’ interest in training on treatment innovations and health disparities. Over two-thirds of providers already offer long-acting injectable treatments for HIV, indicating a willingness to adopt innovative approaches. There is an opportunity to provide more medical education that is responsive to current workforce needs, fostering expansion and innovation in HIV care.
Barrier
Despite treatment innovations, viral suppression among PWH remains at 65% due to ongoing gaps in social and behavioral health services, such as housing insecurity, mental illness, and the opioid epidemic. Despite treatment innovations, viral suppression among PWH remains at 65% due to ongoing gaps in social and behavioral health services, such as housing insecurity, mental illness, and the opioid epidemic.
Opportunity
Expanding behavioral health and social services is essential to addressing these gaps and helping priority populations maintain HIV care while managing co-occurring conditions like mental health issues and substance use. By tackling these intertwined challenges, we can improve long-term health outcomes and support viral suppression.
Barrier
Patients continue to face barriers to treatment access. Providers report that insurance and payor barriers keep patients from accessing regular HIV care and new therapies and directly affects the health outcomes of their clients.
Opportunity
Healthcare organizations and systems need sustained funding to provide support services, as well as expanded insurance coverage and reforms to ensure clients have continuous access to HIV care.







HealthHIV Research and Evaluation conducts regular national surveys to better inform ongoing advocacy, education, research, and training activities. These “State Of” surveys provide unique insight into patient and provider issues in order to optimize primary and support services for diverse communities. The regular reports offer the ability to study multi-year trend analyses illustrating changes, challenges, and opportunities to address the needs of providers and patients. HealthHIV, HealthHCV and the National Coalition for LGBTQ Health conduct State of surveys addressing HIV care, HCV care, LGBTQ healthcare, and aging with HIV.
Appendix: State of HIV Care Survey Data
Organization Background
| Response | Percentage |
|---|---|
| Academic Hospital/Clinic | 7.67% |
| Addiction Center | .57% |
| Advocacy Organization | 1.28% |
| AIDS Service Organization (ASO) | 6.39% |
| Community Based Organization (CBO) | 18.4% |
| Community Center | 1.85% |
| Community Pharmacy | .85% |
| Emergency Room/Urgent Care | .28% |
| Federally Qualified Health Center (FQHC) | 16.05% |
| Government Entity (Local, State, Federal) | 6.96% |
| Health Department (Non-Clinic) | 2.70% |
| Health Department (Clinic/Public Health Clinic) | 11.22% |
| LGBTQ Health Center | 2.13% |
| Other | 4.97% |
| Private Hospital/Clinic | 2.13% |
| Private Practice | 2.13% |
| Ryan White HIV/AIDS Program Clinic | 11.65% |
| Specialty Pharmacy | .71% |
| Substance Use Treatment Facility | .71% |
| University/College | 1.28% |
| Veterans Affairs Medical Center | .43% |
| Response | Percentage | Count |
|---|---|---|
| Alabama | 1.29% | 9 |
| Alaska | .86% | 6 |
| Arizona | 2.00% | 14 |
| Arkansas | .86% | 6 |
| California | 6.71% | 47 |
| Colorado | .86% | 6 |
| Connecticut | 1.86% | 13 |
| Delaware | .86% | 6 |
| District of Columbia | 2.71% | 19 |
| Florida | 10.00% | 70 |
| Georgia | 2.86% | 20 |
| Hawaii | .14% | 1 |
| I do not live/work in the U.S. | 1.71% | 12 |
| Idaho | .29% | 2 |
| Illinois | 3.71% | 26 |
| Indiana | 1.57% | 11 |
| Iowa | .14% | 1 |
| Kansas | .57% | 4 |
| Kentucky | 1.29% | 9 |
| Louisiana | 2.29% | 16 |
| Maine | .14% | 1 |
| Massachusetts | 2.57% | 18 |
| Michigan | 4.43% | 31 |
| Mississippi | 1.00% | 7 |
| Missouri | 1.71% | 12 |
| Montana | .43% | 3 |
| Nebraska | .14% | 1 |
| Nevada | .71% | 5 |
| New Hampshire | .29% | 2 |
| New Jersey | 2.57% | 18 |
| New Mexico | .29% | 2 |
| New York | 8.57% | 60 |
| North Carolina | 2.71% | 19 |
| Ohio | 2.14% | 15 |
| Oklahoma | .43% | 3 |
| Oregon | .57% | 4 |
| Pennsylvania | 3.57% | 25 |
| Puerto Rico | .86% | 6 |
| Rhode Island | .29% | 2 |
| South Carolina | 3.00% | 21 |
| Tennessee | .57% | 4 |
| Texas | 4.00% | 28 |
| Utah | .29% | 2 |
| Virginia | 2.86% | 20 |
| Washington | 2.14% | 15 |
| West Virginia | 1.29% | 9 |
| Wisconsin | .86% | 6 |
| Wyoming | .71% | 5 |
| Setting (Select all that apply) | Count |
|---|---|
| Urban | 488 |
| Rural | 203 |
| Suburban | 175 |
| Tribal | 13 |
| Response | Percentage |
|---|---|
| No | 53.12% |
| Yes | 46.88% |
| Response | Percentage | Count |
|---|---|---|
| Medicaid | 56.11% | 542 |
| Medicare | 52.07% | 503 |
| Other Public Insurance | 43.69% | 422 |
| Employer-Sponsored Insurance | 43.17% | 417 |
| Other Private Insurance | 45.86% | 443 |
| Income Dependent/Sliding Scale | 39.75% | 384 |
| Other | 15.32% | 148 |
Services Offered
| Response | Percentage | Count |
|---|---|---|
| Preventative Health Screening | 48.76% | 471 |
| Immunizations and Vaccinations | 46.69% | 451 |
| Medication Management/Prescriptions | 43.06% | 416 |
| Management of Chronic Conditions | 41.72% | 403 |
| Annual Exams or Physical Exams | 40.58% | 392 |
| Medicare Wellness Visits | 28.88% | 279 |
| Minor In-Office Surgical Procedures | 15.84% | 153 |
| None of the Above | 11.39% | 110 |
| Other | 8.59% | 83 |
| Response | Percentage |
|---|---|
| No | 29.39% |
| Yes | 70.61% |
| Response | Percentage |
|---|---|
| No | 31.92% |
| Yes | 68.08% |
| Response | Percentage |
|---|---|
| No | 40.35% |
| Yes | 59.65% |
| Response | Percentage |
|---|---|
| No | 21.82% |
| Yes | 78.18% |
| Response | Percentage | Count |
|---|---|---|
| HIV Prevention Education | 58.70% | 567 |
| HIV Testing | 57.87% | 559 |
| Linkage to Care/Treatment | 57.04% | 551 |
| Condom Distribution | 56.31% | 544 |
| Provision of PrEP | 50.52% | 488 |
| Behavioral Risk Reduction Interventions | 48.14% | 465 |
| Partner Services | 40.68% | 393 |
| Provision of nPEP | 38.61% | 373 |
| Other | 4.14% | 1 |
| Response | Percentage | Count |
|---|---|---|
| STI Screening and Testing | 57.56% | 556 |
| HPV Screening or Vaccinations | 43.06% | 416 |
| Viral Hepatitis (A, B) Services (including vaccination) | 42.34% | 409 |
| Family Planning Services | 30.54% | |
| Gender Affirming Services | 25.26% | 244 |
| Expedited Partner Therapy (EPT) | 22.36% | 216 |
| None of the Above | 10.04% | 97 |
| Other | 3.52% | 34 |
| Response | Percentage | Count |
|---|---|---|
| Case Management | 52.07% | 503 |
| Transportation Services (bus passes, ride share, etc.) | 47.31% | 457 |
| Health Care Insurance Navigation (ACA plans, SSDI/SSI, etc.) | 38.61% | 373 |
| Food/Nutrition Services (food pantry, food stamps, etc.) | 36.85% | 356 |
| Housing Services | 28.67% | 277 |
| None of the Above | 7.45% | 72 |
| Child Care | 3.52% | 34 |
| Other | 3.52% | 34 |
| Response | Percentage | Count |
|---|---|---|
| Individual Psychotherapy/Counseling | 39.65% | 383 |
| Peer-Led Support Groups | 26.81% | 259 |
| Outpatient Medicine Management | 26.60% | 257 |
| Group Psychotherapy/Counseling | 21.84% | 211 |
| Medication Assisted Treatment (MAT) | 21.12% | 204 |
| None of the Above | 13.56% | 131 |
| Crisis Support/Hotlines | 12.84% | 124 |
| Syringe Exchange Services | 11.80% | 114 |
| Inpatient Treatment | 9.73% | 94 |
| Intensive Outpatient Services (IOP) | 7.76% | 75 |
| Inpatient Detox Services | 3.93% | 38 |
| Other | 2.90% | 28 |
Populations Served
| Response | Percentage | Count |
|---|---|---|
| Adults (25-49) | 65.94% | 637 |
| Older Adults (50+) | 62.84% | 607 |
| Youth (18-24) | 60.35% | 583 |
| Children and Adolescents (Under 17) | 33.13% | 320 |
| Response | Percentage | Count |
|---|---|---|
| Gay Men/Men Who Have Sex With Men (MSM) | 66.46% | 642 |
| People Who Identify as Bisexual | 65.32% | 631 |
| People Who Identify as Transgender | 63.77% | 616 |
| Lesbians/Women Who Have Sex With Women (WSW) | 62.84% | 607 |
| People Who Identify as Queer | 62.84% | 607 |
| People Who Identify as Non-Binary | 61.59% | 595 |
| None | 2.17% | 21 |
| Response | Percentage | Count |
|---|---|---|
| People Experiencing Homelessness/Unhoused | 62.53% | 604 |
| People with Substance Use Disorders | 62.01% | 599 |
| Non-English-Speaking Individuals | 60.04% | 580 |
| Women of Childbearing Age | 58.07% | 561 |
| People Who Are Incarcerated or Formerly Incarcerated | 56.83% | 549 |
| Immigrants/Refugees | 54.87% | 530 |
| Undocumented Persons | 54.35% | 525 |
| Pregnant Women | 50.72% | 490 |
| None of the Above | 1.55% | 15 |
Participant Professional Background
| Response | Percentage |
|---|---|
| Clinical | 39.09% |
| Non-Clinical | 60.91% |
| Response | Percentage |
|---|---|
| Dentist | 1.87% |
| Dietician/Nutritionist | .37% |
| Endocrinologist | .37% |
| Licensed Clinical Social Worker | 3.75% |
| Licensed Practical Nurse | 5.62% |
| Medical Assistant | 3.37% |
| Mental Health Case Manager | 1.12% |
| Mental Health Professional | 5.24% |
| Nurse Manager | 4.12% |
| Nurse Practitioner | 18.35% |
| Occupational Therapist | .37% |
| Other Provider/Clinical Professional | 7.12% |
| Pharmacist | 7.12% |
| Physician (MD/DO) | 18.35% |
| Physician Associate | 3.75% |
| Registered Nurse | 19.10% |
| Response | Percentage | Count |
|---|---|---|
| Addiction Medicine/Substance Use | 3.00% | 29 |
| Cardiology | .21% | 2 |
| Correctional Medicine | .31% | 3 |
| Diabetology | .21% | 2 |
| Emergency Medicine | .41% | 4 |
| Endocrinology | .21% | 2 |
| Family Medicine | 5.69% | 55 |
| Gastroenterology | .10% | 1 |
| Hematology | .21% | 2 |
| Hepatology | .72% | 7 |
| HIV Medicine | 10.56% | 102 |
| Infectious Disease | 8.70% | 84 |
| Internal Medicine | 3.31% | 32 |
| Managed Care | .52% | 5 |
| OBGYN/Women’s Health | 1.66% | 16 |
| Oncology | .41% | 4 |
| Pediatrics | 1.97% | 19 |
| Pharmacy | 1.14% | 11 |
| Primary Care | 3.93% | 38 |
| Psychiatry/Behavioral Health | 2.69% | 26 |
| Pulmonology | .21% | 2 |
| Rheumatology | .10% | 1 |
| Other | 2.38% | 23 |
| None of the Above | 1.76% | 17 |
| Response | Percentage |
|---|---|
| No | 55.81% |
| Yes | 44.19% |
| Response | Percentage |
|---|---|
| Administrator | 22.36% |
| Advocate | 4.81% |
| Case Manager/Medical Case Manager | 17.07% |
| Clergy/Faith-Based Professional | .24% |
| Community Health Worker | 12.02% |
| Disease Intervention Specialist | 3.13% |
| Harm Reductionist/Risk Reductionist | 2.40% |
| Health Education Specialist | 5.77% |
| Health Navigator | 4.09% |
| Medical Billing | .72% |
| Mental Health Professional | .72% |
| Non-Clinical Professional | 12.26% |
| Outreach Worker | 5.77% |
| Researcher | 3.13% |
| Student | .24% |
| Substance Use Counselor/Professional | .72% |
| Response | Percentage |
|---|---|
| Less Than 2 Years | 19.50% |
| 11-20 Years | 20.53% |
| 2-4 Years | 21.99% |
| 21+ Years | 17.89% |
| 5-10 Years | 20.09% |
Participant Demographics
| Response | Percentage |
|---|---|
| Female/Woman | 65.38% |
| Genderqueer/Gender Non-Conforming/Non-Binary | 3.57% |
| Male/Man | 27.19% |
| Prefer Not to Respond | 1.93% |
| Prefer to Self-Describe | .59% |
| Transgender Man | .89% |
| Transgender Woman | .45% |
| Response | Percentage |
|---|---|
| Asian and/or Asian American | 1.79% |
| Black or African American | 31.49% |
| Multiracial | 7.16% |
| Native American or Alaska Native | .60% |
| Native Hawaiian or Pacific Islander | .15% |
| Prefer Not to Respond | 5.97% |
| Prefer to Self-Describe | 2.69% |
| White or Caucasian | 50.15% |
| Response | Percentage |
|---|---|
| No | 79.20% |
| Prefer Not to Respond | 3.86% |
| Yes | 16.94% |
| Response | Percentage |
|---|---|
| 18–24 | 1.49% |
| 25–34 | 11.89% |
| 35–44 | 21.84% |
| 45–54 | 24.67% |
| 55–64 | 25.71% |
| 65+ | 11.29% |
| Prefer Not to Respond | 3.12% |
Workforce Burnout
| Response | Percentage |
|---|---|
| A Few Times a Month | 23.86% |
| A Few Times a Week | 15.32% |
| A Few Times a Year or Less | 24.45% |
| Every Day | 6.92% |
| Never | 7.51% |
| Once a Month or Less | 13.11% |
| Once a Week | 8.84% |
| Response | Percentage |
|---|---|
| No | 55.60% |
| Yes | 44.40% |
| Response | Percentage |
|---|---|
| A Few Times a Month | 21.18% |
| A Few Times a Week | 26.18% |
| A Few Times a Year or Less | 6.03% |
| Every Day | 30.44% |
| Never | .74% |
| Once a Month or Less | 7.79% |
| Once a Week | 7.65% |
| Response | Percentage |
|---|---|
| Agree | 41.79% |
| Disagree | .90% |
| Neutral | 8.51% |
| Strongly Agree | 46.42% |
| Strongly Disagree | 2.39% |
| Response | Percentage |
|---|---|
| Agree | 44.25% |
| Disagree | 3.14% |
| Neutral | 13.75% |
| Strongly Agree | 36.32% |
| Strongly Disagree | 2.54% |
| Response | Percentage |
|---|---|
| Agree | 41.77% |
| Disagree | 5.39% |
| Neutral | 17.07% |
| Strongly Agree | 30.99% |
| Strongly Disagree | 4.79% |
| Response | Count |
|---|---|
| Workforce Shortage | 155 |
| Poor and/or Stagnant Compensation | 149 |
| Burnout | 70 |
| Inflexible Work Shifts/Scheduling | 17 |
| Lack of Training | 23 |
| Inadequate Benefits Package | 21 |
| Inadequate Paid Time Off/Vacation | 18 |
| Increased Workload | 93 |
| Response | Percentage |
|---|---|
| Incorporating More Mental/Behavioral Health Services for Staff | 17.08% |
| Allowing More Flexible Schedules | 23.50% |
| Creating a Crisis Hotline | 2.90% |
| Ensuring Adequate Staffing | 19.46% |
| Supporting Manageable Workloads | 22.77% |
| Promoting Social Experiences Among Staff | 19.67% |
| Working to Improve Bureaucratic Processes | 14.08% |
| Other | 3.62% |
| None of the Above | 17.08% |
Education and Training
| Response | Percentage |
|---|---|
| Online Conferences/Meetings | 5.07% |
| Webinars | 51.35% |
| In-Person Conferences/Meetings | 48.03% |
| Self-Paced Courses (online) | 46.48% |
| Internal Organizational Training (in-person) | 34.47% |
| Self-Paced Educational Videos | 31.88% |
| Self-Paced Microlearning | 11.18% |
| Social Media | 10.35% |
| Self-Paced Simulations | 6.31% |
| Other | 2.80% |
| None of the Above | .10% |
| Response | Percentage |
|---|---|
| In-Person Conferences/Meetings | 48.96% |
| Online Conferences/Meetings | 37.16% |
| Webinars | 36.96% |
| Self-Paced Courses (online) | 36.96% |
| Internal Organizational Training (in-person) | 25.05% |
| Self-Paced Educational Videos | 20.60% |
| Self-Paced Microlearning | 9.73% |
| Self-Paced Simulations | 9.94% |
| Social Media | 5.69% |
| Other | 1.35% |
| None of the Above | 0% |
| Response | Count |
|---|---|
| Monitoring Health Disparities/Addressing Health Equity | 122 |
| Fiscal Health (Ryan White, 340B, PrEP) | 56 |
| Preventing Stigma and Discrimination | 55 |
| Addressing Mental/Behavioral Health | 48 |
| Providing Trauma Informed Care | 40 |
| Discussing Sexual Health with Clients/Patients | 34 |
| Addressing Structural Racism | 33 |
| Providing Culturally Competent Care | 29 |
| Preventing Provider Burnout/Health Care Workforce Shortages | 27 |
| Building Coalitions/Patient Access Advocacy | 21 |
| Providing Affirmative Care for Transgender/Non-Binary Clients | 17 |
| Discussing Substance Use with Clients/Patients | 15 |
| Conducting Motivational Interviewing | 13 |
| Caring for Undocumented Individuals | 11 |
| Expanding/Implementing Telehealth | 11 |
| Conducting Risk Assessments | 10 |
| Immunizations/Vaccinations | 10 |
| Other | 10 |
| Increasing Workforce Diversity | 7 |
| Response | Count |
|---|---|
| New HIV Treatments Including Injectable Treatment | 113 |
| Integration of STIs, Viral Hepatitis, and HIV Services | 41 |
| Current HIV Treatment Guidelines | 40 |
| Reducing Administrative Burdens Related to Treatment Prior Authorizations | 37 |
| Integrating HIV Treatment into Primary Care | 35 |
| Monitoring Clients/Patients with HIV Not on Treatment | 32 |
| Addressing Treatment Resistance Among Clients/Patients with HIV | 31 |
| Discussing Management of HIV Treatment Side Effects | 23 |
| Ordering and Interpreting Baseline HIV Labs | 14 |
| Managing HCV Coinfection with HIV | 11 |
| Managing HBV Coinfection with HIV | 6 |
| Other | 2 |
| Response | Count |
|---|---|
| Providing On-Demand PrEP/PrEP 211 | 75 |
| Providing PrEP for Hard to Reach Populations | 56 |
| Providing Injectable PrEP | 35 |
| Applying a “Whole Person” Approach to PrEP Programs | 30 |
| Promoting PrEP Programs in the Community | 29 |
| Funding PrEP Programs | 27 |
| Helping Clients/Patients Cover the Costs of PrEP | 18 |
| Providing TelePrEP Services | 14 |
| Providing Event-Based PrEP | 13 |
| Linking Clients from PEP to PrEP | 12 |
| Providing PrEP in the Pharmacy Setting | 11 |
| Providing PrEP Navigation Services | 11 |
| Linking Clients from PrEP to Doxy PEP | 9 |
| Assessing Behavioral Risk/Taking a Sexual History | 6 |
| Navigating Reimbursement for PrEP Services | 6 |
| Other | 2 |
Primary Care
| Response | Percentage |
|---|---|
| No | 78.03% |
| Yes | 21.97% |
| Response | Percentage |
|---|---|
| Cardiovascular Disease (e.g., Hypertension, Cholesterol) | 83.18% |
| Diabetes Screening (e.g., Fasting Glucose, A1C) | 83.18% |
| Frailty Screening (e.g. Bone Density Scan) | 60.75% |
| None of the Above | 14.02% |
| Response | Percentage |
|---|---|
| I Perform This Screening | 36.79% |
| I Refer My Clients/Patients to Another Provider for This Screening | 46.23% |
| This Screening is Not Part of My Standard of Care | 16.98% |
| Response | Percentage |
|---|---|
| I Perform This Screening | 29.52% |
| I Refer My Clients/Patients to Another Provider for This Screening | 53.33% |
| This Screening is Not Part of My Standard of Care | 17.14% |
| Response | Percentage |
|---|---|
| I Perform This Screening | 63.21% |
| I Refer My Clients/Patients to Another Provider for This Screening | 27.36% |
| This Screening is Not Part of My Standard of Care | 9.43% |
| Response | Percentage |
|---|---|
| I Perform This Screening | 49.06% |
| I Refer My Clients/Patients to Another Provider for This Screening | 30.19% |
| This Screening is Not Part of My Standard of Care | 20.75% |
| Response | Percentage |
|---|---|
| I Perform This Screening | 61.68% |
| I Refer My Clients/Patients to Another Provider for This Screening | 20.56% |
| This Screening is Not Part of My Standard of Care | 17.76% |
| Response | Percentage |
|---|---|
| I Perform This Screening | 33.02% |
| I Refer My Clients/Patients to Another Provider for This Screening | 43.40% |
| This Screening is Not Part of My Standard of Care | 23.58% |
| Response | Percentage |
|---|---|
| Depression | 82.24% |
| Substance Use | 75.70% |
| Anxiety | 74.77% |
| Self Harm/Suicide Risk | 70.09% |
| Gender Dysphoria | 36.45% |
| Body Dysmorphia | 19.63% |
| None of the Above | 12.15% |
Mpox
| Response | Percentage |
|---|---|
| No | 55.61% |
| Yes | 44.39% |
| Response | Percentage |
|---|---|
| No | 15.47% |
| Unsure | 19.62% |
| Yes | 64.91% |
| Response | Percentage |
|---|---|
| Concerns About Vaccine Pain/Scarring | 1.51% |
| Concerns About Vaccine Safety | 10.94% |
| Cultural/Religious Reasons | .75% |
| Lack of Knowledge About mpox Transmission and/or Vaccine | 37.74% |
| Low Assumption of Infection Risk | 29.43% |
| Medical Mistrust | 10.57% |
| None of the Above | 4.91% |
| Other | 4.15% |
| Response | Percentage |
|---|---|
| No | 16.73% |
| Unsure | 26.24% |
| Yes | 57.03% |
| Response | Percentage |
|---|---|
| No | 49.43% |
| Yes | 50.57% |
Behavioral Health Care
| Response | Percentage |
|---|---|
| No | 80.84% |
| Yes | 19.16% |
| Response | Percentage |
|---|---|
| Depression, Anxiety, Suicidal Ideation | 7.25% |
| Alcohol Use | 6.21% |
| Substance Misuse (Non-Opioid) | 5.28% |
| Post Traumatic Stress Disorder/Trauma | 4.45% |
| Opioid Misuse | 4.35% |
| Smoking/Vaping/Tobacco Use/Cessation | 4.35% |
| Gender Dysphoria | 3.52% |
| Interpersonal Violence | 3.52% |
| Eating Disorders | 2.38% |
| Body Dysmorphia | 1.97% |
| Other | 1.04% |
| None of the Above | .31% |
Sexual and Reproductive Health Care
| Response | Percentage |
|---|---|
| No | 62.90% |
| Yes | 37.10% |
| Response | Percentage |
|---|---|
| No | 7.49% |
| Yes | 92.51% |
| Response | Percentage |
|---|---|
| Annually | 8.09% |
| At Each Visit | 48.55% |
| Every Three Months | 28.90% |
| Every Six Months | 2.89% |
| Other | 11.56% |
| Response | Percentage |
|---|---|
| No | 10.16% |
| Unsure | 9.09% |
| Yes | 80.75% |
| Response | Percentage |
|---|---|
| Pregnancy Testing | 79.68% |
| Birth Control Management | 61.50% |
| Pregnancy Counseling | 54.01% |
| None of the Above | 13.90% |
| Genetic Counseling and Testing | 11.23% |
| Infertility Services | 10.70% |
| Male and Female Sterilization | 9.09% |
| Other | 5.35% |
| Response | Percentage |
|---|---|
| No | 28.88% |
| Unsure | 10.16% |
| Yes | 60.69% |
| Response | Percentage |
|---|---|
| No | 25.13% |
| Unsure | 19.79% |
| Yes | 55.08% |
| Response | Percentage |
|---|---|
| Not Very Comfortable | 1.07% |
| Somewhat Comfortable | 19.25% |
| Very Comfortable | 77.54% |
| Very Uncomfortable | 2.14% |
| Response | Percentage |
|---|---|
| All of the Above | 68.45% |
| STI Protection | 28.89% |
| Sexual Partners | 27.81% |
| Sexual Practices | 25.67% |
| Past History of STIs | 25.67% |
| Pregnancy Intentions/Birth Control | 17.11% |
| Screen for Sexual Violence/Interpersonal Violence | 13.90% |
| Other | 1.07% |
| None of the Above | 0% |
HIV Continuum
| Response | Percentage |
|---|---|
| No | 44.37% |
| Yes | 55.63% |
| Response | Percentage |
|---|---|
| Onsite at My Organization’s Location | 21.74% |
| Community Health Fairs/Events | 15.84% |
| Community Based Organizations (CBOs) | 9.94% |
| At Home Testing | 6.42% |
| Health Department Clinics | 5.28% |
| Substance Use Treatment Centers | 5.18% |
| Correctional Facilities | 4.66% |
| Primary Care Office | 4.55% |
| AIDS Service Organizations (ASOs) | 3.11% |
| Family Planning Clinics | 2.80% |
| Emergency Room/Urgent Care | 1.45% |
| Other | 1.97% |
| Response | Count |
|---|---|
| Refusal to Get Tested | 74 |
| Limited Staff/Workforce Shortage | 47 |
| Limited Testing Resources | 41 |
| Limited Time During Appointments | 25 |
| Limited Testing Guidelines or Organizational Policies (e.g., patient does not meet criteria for testing) | 12 |
| Inadequate Preparation of Testing Providers | 9 |
| Other | 8 |
| Response | Count |
|---|---|
| Fear of Stigma or Discrimination | 107 |
| Assumption of Low HIV Risk | 44 |
| Lack of Knowledge About Available Care | 19 |
| Distrust in Health Care System | 16 |
| Fear of Confidentiality Breach | 13 |
| Mental Health Issues | 8 |
| Substance Use | 8 |
| Insufficient Counseling | 7 |
| Cost or Insurance Issues | 5 |
| Interpersonal Violence Concerns | 2 |
| Other | 2 |
| Lack of Transportation to Testing | 1 |
| Response | Percentages |
|---|---|
| No | 51.87% |
| Yes | 48.13% |
| Response | Percentages |
|---|---|
| Less than 50 | 9.48% |
| 1,000–1,999 | 14.66% |
| 2,000+ | 21.55% |
| 501–999 | 20.69% |
| 51–500 | 33.62% |
| Response | Percentages |
|---|---|
| Decreased | 9.57% |
| Increased | 69.57% |
| No Change | 11.30% |
| Unsure | 9.57% |
| Response | Percentages |
|---|---|
| No | 52.89% |
| Yes | 47.11% |
| Response | Percentages |
|---|---|
| Few than 50 | 80.70% |
| 1,000–1,999 | 1.75% |
| 2,000+ | 3.51% |
| 51–500 | 14.04% |
| Response | Percentages |
|---|---|
| Decreased | 12.39% |
| Increased | 32.74% |
| No Change | 37.17% |
| Unsure | 17.70% |
| Response | Percentages |
|---|---|
| No | 45.52% |
| Yes | 54.48% |
| Response | Count |
|---|---|
| Patient Refusal | 64 |
| Limited Appointment Times | 44 |
| Insurance Coverage Concerns | 30 |
| Indirect Costs of Getting an Appointment | 25 |
| Limited Options for HIV Care in Region | 19 |
| Limited Staff/Workforce Shortage | 17 |
| Patient Refusal | 12 |
| Other | 7 |
| Response | Count |
|---|---|
| Fear of Stigma or Discrimination | 107 |
| Lack of Knowledge About Available Care | 21 |
| Cost or Insurance Issues | 14 |
| Distrust in Health Care System | 12 |
| Substance Use | 11 |
| Fear of Confidentiality Breach | 9 |
| Mental Health Issues | 9 |
| Lack of Transportation to Care | 8 |
| Housing Instability | 7 |
| Long Waiting Times for an Appointment | 6 |
| Employment Issues (e.g., shift scheduling) | 5 |
| Lack of Available Care | 5 |
| Insufficient Counseling | 4 |
| Inconvenient Appointment Times | 3 |
| Childcare Issues | 2 |
| Other | 1 |
| Response | Percentages |
|---|---|
| No | 62.50% |
| Yes | 37.50% |
| Response | Percentages |
|---|---|
| Fewer than 50 | 66.67% |
| 1,000–1,999 | 1.15% |
| 2,000+ | 1.15% |
| 501–999 | 3.45% |
| 51–500 | 27.59% |
| Response | Percentages |
|---|---|
| Decreased | 2.30% |
| Increased | 47.13% |
| No Change | 43.68% |
| Unsure | 6.90% |
| Response | Percentages |
|---|---|
| No | 56.22% |
| Yes | 43.78% |
| Response | Count |
|---|---|
| Insurance Barriers (formulary restrictions) | 54 |
| Concerns About ART Side Effects | 48 |
| Administrative Time Involved in Processing Prior Authorizations or Patient Assistance Applications | 24 |
| Concerns About Adherence to ART | 23 |
| Other | 8 |
| Concerns About ART Interactions with Current Medications/Comorbidities | 7 |
| Response | Count |
|---|---|
| Fear of Stigma or Discrimination | 47 |
| Concerns About ART Side Effects | 41 |
| Insurance Barriers/Co-Pays | 39 |
| Mental Health Issues | 12 |
| Fear of Confidentiality Breach | 9 |
| Distrust in Health Care System | 6 |
| Concerns About ART Interactions with Current Medications | 4 |
| Other | 4 |
| Insufficient Counseling | 1 |
| Response | Percentage |
|---|---|
| No | 22.87% |
| Unsure | 7.45% |
| Yes | 69.68% |
| Response | Percentage |
|---|---|
| No | 40.74% |
| Yes | 59.26% |
| Response | Percentage |
|---|---|
| Fewer than 50 | 13.39% |
| 1,000–1,999 | 13.39% |
| 2,000+ | 7.14% |
| 501–999 | 12.50% |
| 51–500 | 53.57% |
| Response | Percentage |
|---|---|
| Decreased | 7.21% |
| Increased | 50.45% |
| No Change | 29.73% |
| Unsure | 12.61% |
| Response | Percentage |
|---|---|
| Fewer than 49% | 22.87% |
| 50–59% | 12.23% |
| 60–69% | 4.79% |
| 70–79% | 10.64% |
| 80–89% | 14.36% |
| 90–99% | 14.36% |
| None/Not Applicable | 6.91% |
| Unsure | 13.83% |
| Response | Percentage |
|---|---|
| Medicaid | 16.04% |
| Medicare | 2.14% |
| Other | .53% |
| Other Public Insurance | 4.81% |
| Private Insurance (ACA Plan) | 6.95% |
| Private Insurance (Employer) | 21.93% |
| Ryan White/ADAP | 10.16% |
| There Is No Difference | 12.83% |
| Unsure | 24.60% |
| Response | Percentage |
|---|---|
| No | 55.32% |
| Yes | 44.68% |
| Response | Count |
|---|---|
| Lack of Transportation to Care | 44 |
| Fear of Stigma or Discrimination | 33 |
| Mental Health Issues | 27 |
| Housing Instability | 19 |
| Cost or Insurance Issues | 13 |
| Substance Use | 11 |
| Employment Issues (e.g., shift scheduling) | 11 |
| Fear of Confidentiality Breach | 9 |
| Inconvenient Appointment Times | 6 |
| Long Waiting Times For an Appointment | 4 |
| Reluctance to Follow Provider’s Advice | 4 |
| Other | 4 |
| Childcare Issues | 3 |
| Incarceration or Legal Detention | 1 |
| Too Sick to Travel to Clinic | 1 |
| Response | Percentage |
|---|---|
| Routinely Contacts Patients Prior to Their Appointment as a Reminder (e.g. phone, email, text) | 18.22% |
| Routinely Follows Up With Patients Who Miss Their Appointments (e.g. phone, email, text) | 17.70% |
| Routinely Reinforces the Value of Follow Up Visits | 16.46% |
| Provides Patient Navigation or Case Management Services (e.g. accompanying to appointments as needed) | 15.42% |
| Systematically Monitors Retention in Care of All HIV Patients (e.g. monitoring visit adherence, gaps in care, visits per interval or time) | 13.98% |
| Provides Telehealth Services | 13.87% |
| Provides Bridge Counseling and/or Re-Engagement Services | 9.83% |
| Offers Flexible Scheduling (walk-in hours) or Extended Clinic Hours (e.g. evenings, weekends) | 9.42% |
| Other | .31% |
| None | .21% |
| Response | Percentage |
|---|---|
| Dissatisfied | 8.47% |
| Neutral | 21.69% |
| Satisfied | 44.97% |
| Very Dissatisfied | 1.06% |
| Very Satisfied | 23.81% |
| Response | Percentage |
|---|---|
| No | 78.53% |
| Yes | 21.47% |
| Response | Percentage |
|---|---|
| Decreased | 26.83% |
| Increased | 12.20% |
| No Change | 53.66% |
| Unsure | 7.32% |
| Response | Percentage |
|---|---|
| No | 55.24% |
| Yes | 4.76% |
| Response | Count |
|---|---|
| Mental Health Issues | 50 |
| Fear of Stigma or Discrimination | 39 |
| Housing Instability | 27 |
| Substance Use | 18 |
| Pharmacy Issues (e.g. late refills) | 27 |
| Incorrect Medication Administration (e.g. missing doses) | 14 |
| Other | 7 |
| Reluctance to Follow Provider’s Advice | 6 |
| Fear of Confidentiality Breach | 4 |
| Employment Issues (e.g. shift scheduling) | 4 |
| Incarceration or Legal Detention | 1 |
| Response | Percentage |
|---|---|
| No | 1.57% |
| Unsure | 1.57% |
| Yes | 96.86% |
| Response | Percentage |
|---|---|
| No | 53.65% |
| Yes | 46.35% |
| Response | Percentage |
|---|---|
| Decreased | 7.95% |
| Increased | 37.50% |
| No Change | 43.18% |
| Unsure | 11.36% |
| Response | Percentage |
|---|---|
| Initial Receipt of Care/Starting ART | 6.54% |
| Linkage to Care | 13.55% |
| None of the Above | 11.92% |
| Retention in Care | 42.99% |
| Testing and Diagnosis | 19.16% |
| Viral Suppression | 5.84% |
| Response | Percentage |
|---|---|
| Access to HIV Related Data | 1.17% |
| Dedicated Insurance or Health Navigation Specialists | 4.91% |
| Fiscal Health/Funding to Support HIV Services | 30.14% |
| Increased Insurance Coverage for HIV Specific Services | 4.67% |
| Increased Reimbursement Rates or Considerations | 3.97% |
| Marketing Resources to Educate the Public About HIV Care | 9.11% |
| More HIV-Focused Training for Providers | 6.07% |
| More Providers Trained in HIV Care | 17.52% |
| None of the Above | 5.61% |
| Other | 3.50% |
| Support Staff to Provide Wraparound Services to HIV Clients/Patients | 13.32% |
| Response | Percentage |
|---|---|
| Resistance Testing | |
| All of the Time | 12.72% |
| Most of the Time | 5.26% |
| None of the Time | 53.07% |
| Some of the Time | 10.53% |
| Unsure | 18.42% |
| Choosing an Atypical ART Regimen in the Setting of Medication Class Resistance | |
| All of the Time | 14.98% |
| Most of the Time | 3.52% |
| None of the Time | 50.66% |
| Some of the Time | 14.54% |
| Unsure | 16.30% |
| Treating Opportunistic Infections (e.g. toxoplasmosis, tuberculosis, Kaposi’s Sarcoma) | |
| All of the Time | 16.81% |
| Most of the Time | 6.19% |
| None of the Time | 39.82% |
| Some of the Time | 21.68% |
| Unsure | 15.49% |
| Treating HIV/HCV Co-Infection | |
| All of the Time | 18.61% |
| Most of the Time | 4.33% |
| None of the Time | 44.16% |
| Some of the Time | 18.18% |
| Unsure | 14.72% |
| HIV Treatment in Pregnancy | |
| All of the Time | 26.11% |
| Most of the Time | 7.52% |
| None of the Time | 38.94% |
| Some of the Time | 12.83% |
| Unsure | 14.60% |
| Response | Percentage | Aging with HIV | 26.50% |
|---|---|
| Stigma and Discrimination | 24.12% |
| Behavioral Health | 24.02% |
| Whole Person Care | 22.05% |
| HIV and Comorbidities | 21.12% |
| Support Services | 18.43% |
| Transgender Health | 18.32% |
| Harm Reduction | 17.60% |
| Systemic Racism | 17.29% |
| Insurance Costs/Issues | 16.87% |
| Trauma Informed Care | 15.84% |
| Multipurpose Prevention Technologies | 10.56% |
| Treatment Resistance | 9.42% |
| Other | 1.35% |
| None | .10% |
| Response | Percentage | I am Aware of Whole Person Care But Have Not Implemented it Into My Practice | 12.18% |
|---|---|
| I am Not Aware of Whole Person Care | 21.78% |
| I Have Fully Integrated Whole Person Care Into My Practice | 37.94% |
| I Have Partially Integrated Whole Person Care Into My Practice | 28.10% |
| Response | Percentage | Large Co-Pays | 19.44% |
|---|---|
| Limited Medication Formularies/Prior Authorizations for Medications | 22.95% |
| Limited or No Coverage for Specialist Care | 15.46% |
| None of the Above | 23.89% |
| Other | 4.68% |
| Prior Authorizations for Tests/Procedures | 13.58% |
PrEP Continuum
| Response | Percentage | No | 50.41% |
|---|---|
| Yes | 49.59% |
| Response | Count | Promoting Interest in PrEP | 52 |
|---|---|
| Developing Community Trust | 46 |
| Promoting Awareness of HIV Risk | 38 |
| Preventing Stigma and/or Discrimination | 27 |
| Providing Sufficient Counseling | 8 |
| Other | 3 |
| Response | Percentage | Men Who Have Sex With Men (MSM) | 16.98% |
|---|---|
| Youth (18–24) | 15.94% |
| People Who Use Substances | 15.32% |
| Older Adults (50+) | 14.91% |
| Transgender People | 14.80% |
| Heterosexual Women | 13.66% |
| People Who Are Experiencing Homelessness/Are Unhoused | 13.46% |
| Non-English-Speaking Individuals | 13.04% |
| Undocumented Persons | 12.42% |
| People Who Are Incarcerated or Formerly Incarcerated (jail or person) | 11.49% |
| Other | .83% |
| Response | Count | People Who Are Experiencing Homelessness/Are Unhoused | 41 |
|---|---|
| Youth (18–24) | 33 |
| People Who Use Substances | 25 |
| Heterosexual Women | 18 |
| People Who Are Incarcerated or Formerly Incarcerated (jail or person) | 11 |
| Non-English-Speaking Individuals | 11 |
| Older Adults (50+) | 7 |
| Undocumented Persons | 7 |
| Men Who Have Sex With Men (MSM) | 7 |
| Transgender People | 7 |
| Other | 5 |
| Response | Percentage | No | 38.67% |
|---|---|
| Yes | 61.33% |
| Response | Percentage | Decreased | 7.21% |
|---|---|
| Increased | 81.98% |
| Unsure | 10.81% |
| Response | Percentage | No | 54.37% |
|---|---|
| Yes | 45.63% |
| Response | Percentage | No | 63.86% |
|---|---|
| Yes | 36.14% |
| Response | Percentage | Fewer Than 50 | 45.00% |
|---|---|
| 1,000 – 1,999 | 5.00% |
| 2,000+ | 1.67% |
| 501 – 999 | 3.33% |
| 51 – 500 | 45.00% |
| Response | Percentage | Decreased | 13.56% |
|---|---|
| Increased | 57.63% |
| No Change | 23.73% |
| Unsure | 5.08% |
| Response | Count | Provider Discomfort Discussion PrEP | 53 |
|---|---|
| Refusal to be Linked to PrEP | 33 |
| Limited Staff/Workforce Shortage at PrEP Clinics | 23 |
| Limited PrEP Clinics/Services | 21 |
| Limited Appointment Times | 13 |
| Other | 8 |
| Limited Guidelines or Organizational Policies (e.g. patient does not meet criteria for PrEP services) | 5 |
| Response | Count | Provider Initiated Patient Discussions | 74 |
|---|---|
| Targeted Community Promotions (e.g. transit signage, billboards, public benches, etc.) | 20 |
| Peer to Peer Discussions | 20 |
| Dating Apps | 16 |
| Influencers/Community Representatives | 8 |
| Provider Presentations/Tabling at Community Social Gathering Events (e.g. Pride events, community center events, faith-based events, etc.) | 7 |
| TV Advertisements | 6 |
| Social Media Marketing | 5 |
| Other | 2 |
| Promotional Materials in Clinic Waiting Rooms | 1 |
| Response | Percentage | No | 71.58% |
|---|---|
| Yes | 28.42% |
| Response | Percentage | Insurance Issues | 5.49% |
|---|---|
| Workflows for Integrating CAB Administration Into Your Practice | 2.69% |
| Funding to Support a CAB Program | 2.17% |
| Access to Adequate Support Staff (PrEP navigators, case managers, etc.) | 1.66% |
| Physical Capacity (e.g. refrigeration units, syringes, etc.) | 1.24% |
| Staff Training | .93% |
| Other | .21% |
| We Have Not Encountered Any Barriers Providing CAB | 0% |
| Response | Percentage | TDF/FTC (Truvada) | 10.46% |
|---|---|
| TAF/FTC (Descovy) | 9.63% |
| CAB (Apretude) | 6.73% |
| Response | Percentage | Private Insurance (employer) | 44.23% |
|---|---|
| There Is No Difference | 22.12% |
| Medicaid | 8.65% |
| Other | 4.81% |
| Medicare | 4.81% |
| Other Public Insurance | 3.85% |
| Ryan White/ADAP | 1.92% |
| Response | Percentage | Very Confident | 62.14% |
|---|---|
| Fairly Confident | 22.33% |
| Somewhat Confident | 11.65% |
| Slightly Confident | 1.94% |
| Not Confident At All | 1.94% |
| Response | Percentage | Routinely/At Every PrEP Visit | 90.91% |
|---|---|
| Only When Symptoms Arise | 9.09% |
| Response | Percentage | Unsure | 24.04% |
|---|---|
| Less Than 49% | 20.19% |
| 50–59% | 15.38% |
| 60-69% | 12.50% |
| 80-89% | 9.62% |
| 70-79% | 8.65% |
| 90-99% | 7.69% |
| None/Not Applicable | 1.92% |
| Response | Percentage | Increased | 62.86% |
|---|---|
| No Change | 14.29% |
| Decreased | 14.29% |
| Unsure | 8.57% |
| Response | Count | Time Required to Complete Prior Authorizations | 34 |
|---|---|
| Preferred PrEP Modality Not Covered by Insurance | 24 |
| No Insurance | 20 |
| Concerns About Adherence to PrEP | 10 |
| Low or No Reimbursement for PrEP Office Visits | 2 |
| Concerns About Medication Interactions | 2 |
| Response | Count | Low Perceived HIV Risk | 36 |
|---|---|
| Fear of Stigma or Discrimination | 19 |
| Cost or Insurance Issues (e.g co-pays) | 17 |
| Insufficient Counseling | 7 |
| Concern About Medication Side Effects | 6 |
| Distrust in Health Care System | 5 |
| Lack of Transportation to Care | 2 |
| Long Waiting Times for an Appointment | 2 |
| Lack of Available Care | 1 |
| Housing Instability | 1 |
| Mental Health Issues | 1 |
| Substance Use | 1 |
| Response | Percentage | No | 65.30% |
|---|---|
| Yes | 34.70% |
| Response | Percentage | Satisfied | 36.36% |
|---|---|
| Neutral | 33.88% |
| Very Satisfied | 18.18% |
| Dissatisfied | 9.92% |
| Very Satisfied | 1.65% |
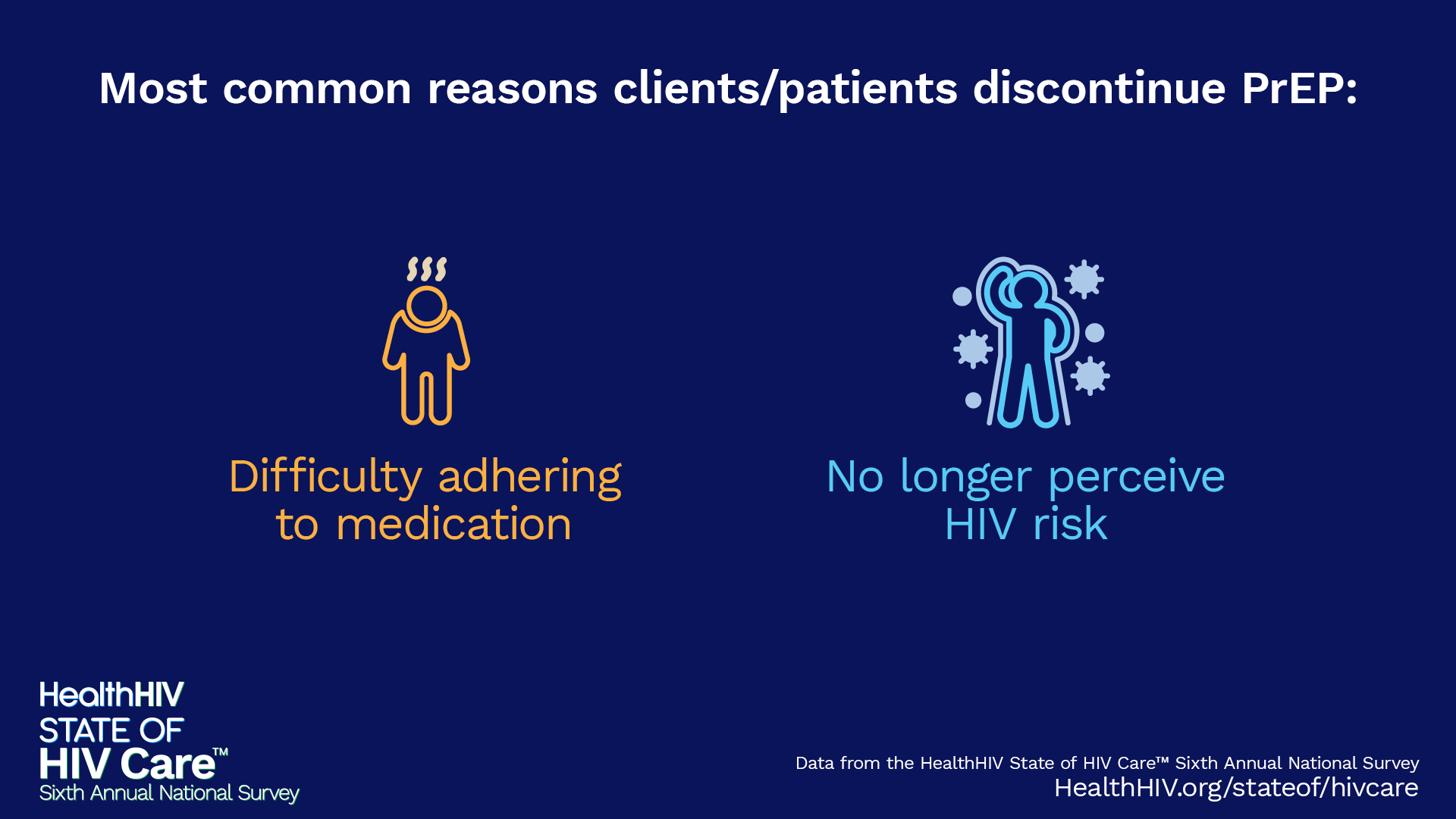
| Response | Count | Difficulty Adhering to Medication | 31 |
|---|---|
| No Longer Perceive HIV Risk | 21 |
| Medication Cost/Lack of Insurance | 19 |
| Frequency of Required Appointments | 18 |
| Appointment Cost | 11 |
| Medication Side Effects | 6 |
| Fear of Stigma or Discrimination | 5 |
| Distance From Nearest Pharmacy | 3 |
| Difficulty Obtaining Refills From the Pharmacy | 2 |
| Other | 2 |
| Response | Percentage | Routinely Contacts Patients Prior to Appointment as a Reminder (e.g. phone, email, text) | 11.18% |
|---|---|
| Routinely Follows Up With Patients Who Miss Appointments (e.g. phone, email, text) | 10.04% |
| Provides PrEP Navigation or Case Management Services | 9.73% |
| Routinely Reinforces Value of Followup Visits | 9.63% |
| Systematically Monitors Retention in Care of All PrEP Patients (e.g. monitoring visit adherence, gaps in care, or visits per interval or time) | 7.76% |
| Response | Percentage | Outreach/PrEP Promotion | 39.34% |
|---|---|
| Retention in Care | 21.58% |
| Linkage to PrEP | 13.39% |
| Adherence to PrEP | 9.56% |
| Prescribing PrEP | 8.47% |
| PrEP Uptake | 7.65% |
| Response | Percentage | No | 74.79% |
|---|---|
| Yes | 25.21% |
| Response | Percentage | No | 47.40% |
|---|---|
| Yes | 52.60% |
Anti-LGBTQ Policies
| Response | Percentage | No | 54.27% |
|---|---|
| Yes | 45.73% |
| Response | Percentage | No | 33.64% |
|---|---|
| Yes | 66.36% |
| Response | Percentage | No | 47.20% |
|---|---|
| Yes | 52.80% |
| Response | Percentage | Always | 3.00% |
|---|---|
| Never | 28.69% |
| Often | 6.00% |
| Rarely | 35.97% |
| Sometimes | 26.34% |
| Response | Percentage | No | 71.95% |
|---|---|
| Yes | 28.05% |
| Response | Percentage | Always | 13.74% |
|---|---|
| Often | 15.27% |
| Rarely | 38.39% |
| Sometimes | 32.06% |
| Response | Percentage | No | 29.34% |
|---|---|
| Yes | 70.66% |
| Response | Percentage |
|---|---|
| Increasing public awareness and understanding of HIV and its impacts, and challenging myths and misconceptions about HIV transmission and criminalization. | 35.09% |
| Educating lawmakers and law enforcement officials on HIV and its transmission. | 33.95% |
| Replacing laws that criminalize HIV exposure, transmission, or non disclosure with public health approaches that prioritize prevention, testing, treatment, and support. | 33.64% |
| Building coalitions and partnerships across sectors and communities to advance policies and practices that reduce HIV related stigma, discrimination, and criminalization. | 31.68% |
| Increasing HIV testing rates by reducing stigma and discrimination against PLWH. | 30.64% |
| Strengthening community based organizations and networks that advocate for the rights PLWH and provide legal and social support services. | 30.43% |
| Response | Percentage |
|---|---|
| NEUTRAL: I do not have a strong opinion on the use of MHS for HIV. I would like to learn more about the technology, its benefits, and its limitations before making a decision. | 37.26% |
| STRONGLY SUPPORT: I believe that MHS is an important tool for tracking the spread of HIV and monitoring the effectiveness of treatments. | 25.05% |
| SOMEWHAT SUPPORT: I think that MHS for HIV has some potential benefits, but it also raises concerns about privacy, data security, and confidentiality. | 23.77% |
| SOMEWHAT OPPOSE: I have some concerns about the potential impact of MHS on individual privacy and confidentiality for PLWH. I believe that any surveillance program should be designed with safeguards to protect the privacy and rights of individuals. | 7.92% |
| STRONGLY OPPOSE: I believe that MHS for HIV is an invasion of privacy and a violation of human rights. Genetic testing should not be used to track the spread of HIV or monitor the effectiveness of treatments, as it can stigmatize and marginalize PLWH and undermine their autonomy and dignity. | 6.00% |
| Response | Percentage |
|---|---|
| I Am Not Aware of This Ruling | 54.93% |
| No | 43.10% |
| Yes | 1.97% |
| Response | Percentage |
|---|---|
| No | 52.96% |
| Yes | 47.04% |
| Response | Percentage |
|---|---|
| No | 63.35% |
| Yes | 36.65% |
| Response | Percentage |
|---|---|
| No | 6.52% |
| Yes | 93.48% |
| Response | Percentage |
|---|---|
| No | 10.12% |
| Unsure | 40.08% |
| Yes | 49.80% |
| Response | Percentage |
|---|---|
| No | 94.05% |
| Yes | 5.95% |
| Response | Percentage |
|---|---|
| No | 72.97% |
| Yes | 27.03% |
| Response | Percentage |
|---|---|
| No | 4.55% |
| Yes | 95.45% |
Notes
- Centers for Disease Control and Prevention. (2024, June 10). Ending the HIV Epidemic in the US Jurisdictions and Plans. Ending the HIV Epidemic in the US (EHE). https://www.cdc.gov/ehe/php/jurisdictions-plans/index.html
- Centers for Disease Control and Prevention. (2024, May 14). About Ending the HIV Epidemic in the US. Ending the HIV Epidemic in the US (EHE). https://www.cdc.gov/ehe/php/about/index.html
- Collins, S. R., Haynes, L. A., & Masitha, R. (2022, September 29). State of U.S. Health Insurance in 2022: Biennial Survey. The Commonwealth Fund. https://www.commonwealthfund.org/publications/issue-briefs/2022/sep/state-us-health-insurance-2022-biennial-survey
- Centers for Disease Control and Prevention. (2024, July 1). Fast Facts: HIV in the United States. HIV. https://www.cdc.gov/hiv/data-research/facts-stats/index.html
- National Center for Health Workforce Analysis. (2023). Behavioral Health Workforce, 2023. HRSA. https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/Behavioral-Health-Workforce-Brief-2023.pdf
- Bridging the Gap: The Urgent Need for Social Workers. (2023, September 29). Columbia School of Social Work Blog. https://socialwork.columbia.edu/news/bridging-gap-urgent-need-social-workers
- Nachega, J. B., Scarsi, K. K., Gandhi, M., Scott, R. K., Mofenson, L. M., Archary, M., Nachman, S., Decloedt, E., Geng, E. H., Wilson, L., Rawat, A., & Mellors, J. W. (2023). “Long-acting antiretrovirals and HIV treatment adherence.” The Lancet HIV, 10(5), e332–e342.
- Crawford, N. D., Lewis, C. F., Moore, R., Pietradoni, G., & Weidle, P. (2022). “Examining the Multilevel Barriers to Pharmacy-Based HIV Prevention and Treatment Services.” Sexually Transmitted Diseases, 49(11S), S22. https://doi.org/10.1097/OLQ.0000000000001643
- Cooper, V., Clatworthy, J., Whetham, J., & Consortium, E. (2017). “mHealth Interventions To Support Self-Management In HIV: A Systematic Review.” The Open AIDS Journal, 11, 119–132. https://doi.org/10.2174/1874613601711010119
- Reinert, M., Fritze, D., & Nguyen, T. (2022). “The State of Mental Health in America 2023.” Mental Health America.
- Centers for Disease Control and Prevention. (2024, June 10). Ending the HIV Epidemic in the US Jurisdictions and Plans. Ending the HIV Epidemic in the US (EHE). https://www.cdc.gov/ehe/php/jurisdictions-plans/index.htm
- Menza, T. W., Berry, S. A., Dombrowski, J., Cachay, E., Crane, H. M., Kitahata, M. M., & Mayer, K. H. (2022). “Anatomic Site–Specific Gonorrhea and Chlamydia Testing and Incidence Among People With HIV Engaged in Care at 4 US Clinical Centers, 2014–2018.” Open Forum Infectious Diseases, 9(7), ofac298. https://doi.org/10.1093/ofid/ofac298
- Bachmann, L. H. (2024). “CDC Clinical Guidelines on the Use of Doxycycline Postexposure Prophylaxis for Bacterial Sexually Transmitted Infection Prevention, United States, 2024.” MMWR. Recommendations and Reports, 73. https://doi.org/10.15585/mmwr.rr7302a1
- Centers for Disease Control and Prevention. (2023, November 3). Expedited Partner Therapy. https://www.cdc.gov/std/ept/default.htm
- Harsono, D., Galletly, C. L., O’Keefe, E., & Lazzarini, Z. (2017). “Criminalization of HIV exposure: a review of empirical studies in the United States.” AIDS and Behavior, 21, 27-50. https://link.springer.com/article/10.1007/s10461-016-1540-5
- Hoppe, T. , McClelland, A. & Pass, K. (2022). “Beyond criminalization: reconsidering HIV criminalization in an era of reform.” Current Opinion in HIV and AIDS, 17 (2), 100-105. https://doi.org/10.1097/COH.0000000000000715
- Keralis, J. M. (2023). “HIV Criminalization Laws and Enforcement: Assessing the Relationship Between HIV Criminalization at the State Level, Policing at the County Level, and County-level HIV Incidence Rates.” AIDS and Behavior, 27(11), 3713–3724. https://doi.org/10.1007/s10461-023-04087-z
- https://pubmed.ncbi.nlm.nih.gov/32211784/
- Human Rights Campaign. (2024). Map: Attacks on Gender Affirming Care by State. https://www.hrc.org/resources/attacks-on-gender-affirming-care-by-state-map

HealthHIV is a national non-profit working with healthcare organizations, communities, and providers to advance effective HIV and HCV prevention, care, and support through education and training, technical assistance and capacity building, advocacy, communications, and health services research and evaluation.
1630 Connecticut Avenue NW, Suite 500 • Washington, DC 20009
202-232-6749 • HealthHIV.org
120324B
